

Outcomes of a Standardized, High-Caloric, Inpatient Re-Alimentation Treatment Protocol in 120 Severely Malnourished Adolescents with Anorexia Nervosa
- PMID: 35566710
- PMCID: PMC9105338
- DOI: 10.3390/jcm11092585
Outcomes of a Standardized, High-Caloric, Inpatient Re-Alimentation Treatment Protocol in 120 Severely Malnourished Adolescents with Anorexia Nervosa
Abstract
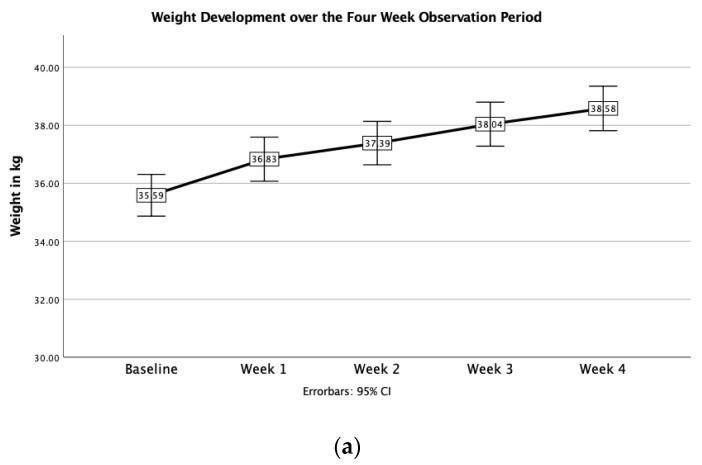
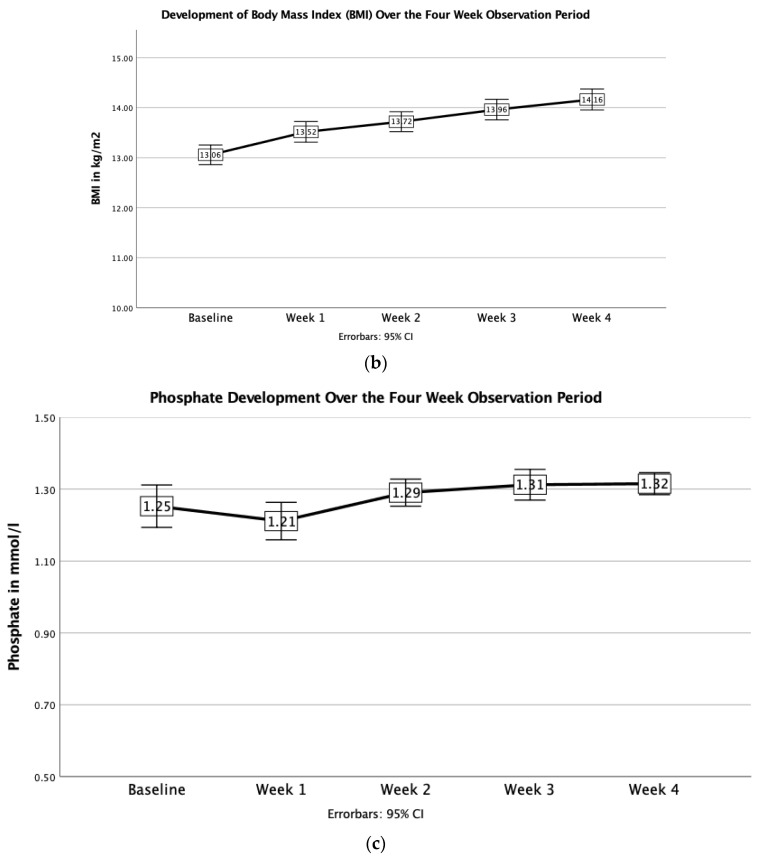
Evidence accumulates that, with close medical monitoring and phosphate supplementation, higher-caloric re-alimentation protocols beginning at 2000 kcal/day (HCR) are not associated with an increased incidence of electrolyte abnormalities in patients with anorexia nervosa (AN) but rather result in faster weight gain. These studies are still scant and have largely been performed in adults or moderately malnourished adolescents. Methods: A retrospective chart review of patients with AN aged 12−20 years and with a body mass index (BMI) < 15 kg/m2 alimented according to a standardized treatment protocol in a German clinic specialized in AN was conducted. All patients received 2000 kcal/day from day one. The effect of HCR was examined with respect to laboratory changes and weight development over 4 weeks. Results: In 120 youth (119 (99.2%) females and 1 (0.8%) male, the mean BMI was 13.1 ± 1.1 (range = 10.2−15.0), %mBMI was 62.1 ± 6.0% and weight gain was 0.76 ± 0.22 kg per week, with the highest rate of weight gain during week 1 (1.25 ± 1.28 kg/week). Over 4 weeks, the total weight gain was 3.00 ± 1.92 kg. Nine patients (7.5%) developed mild hypophosphatemia, and none developed refeeding syndrome. Conclusions: Starting re-alimentation with 2000 kcal/d under close medical surveillance, severely malnourished youth with AN met the recommended weight gain targets between 0.5 and 1 kg/week according to current treatment guidelines, without anyone developing refeeding syndrome.
Keywords: eating disorders; energy intake; nutrition; refeeding syndrome.
Conflict of interest statement
Correll has been a consultant and/or advisor to or has received honoraria from: AbbVie, Acadia, Alkermes, Allergan, Angelini, Aristo, Axsome, Damitsa, Gedeon Richter, Hikma, IntraCellular Therapies, Janssen/J&J, Karuna, LB Pharma, Lundbeck, MedAvante-ProPhase, MedInCell, Medscape, Merck, Mitsubishi Tanabe Pharma, Mylan, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Relmada, Rovi, Seqirus, Servier, SK Life Science, Sumitomo Dainippon, Sunovion, Supernus, Takeda, Teva and Viatris. He has provided expert testimony for Janssen and Otsuka. He has served on a Data Safety Monitoring Board for Lundbeck, Relmada, Rovi and Teva. He has received grant support from Janssen and Takeda. He has received royalties from UpToDate and is also a stock option holder of LB Pharma. Garber: This study was supported by the National Institutes of Health (R01HD082166), which approved the original design but did not participate in collection, management, analysis, and interpretation of the data; nor preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication. Garber’s time was also supported in part by Health Resources and Services Administration, Leadership Training in Adolescent Health (T71MC00003).
Figures

Similar articles
-
Clinical Outcomes of Refeeding Syndrome: A Systematic Review of High vs. Low-Calorie Diets for the Treatment of Anorexia Nervosa and Related Eating Disorders in Children and Adolescents.Cureus. 2023 May 21;15(5):e39313. doi: 10.7759/cureus.39313. eCollection 2023 May. Cureus. 2023. PMID: 37351245 Free PMC article. Review.
-
Short-term outcomes of the study of refeeding to optimize inpatient gains for patients with atypical anorexia nervosa.Int J Eat Disord. 2024 Apr;57(4):859-868. doi: 10.1002/eat.24115. Epub 2024 Jan 5. Int J Eat Disord. 2024. PMID: 38179719 Free PMC article. Clinical Trial.
-
Higher caloric intake in hospitalized adolescents with anorexia nervosa is associated with reduced length of stay and no increased rate of refeeding syndrome.J Adolesc Health. 2013 Nov;53(5):573-8. doi: 10.1016/j.jadohealth.2013.05.014. Epub 2013 Jul 3. J Adolesc Health. 2013. PMID: 23830088
-
Outcomes of an Accelerated Inpatient Refeeding Protocol in 103 Extremely Underweight Adults with Anorexia Nervosa at a Specialized Clinic in Prien, Germany.J Clin Med. 2020 May 19;9(5):1535. doi: 10.3390/jcm9051535. J Clin Med. 2020. PMID: 32438760 Free PMC article.
-
High-calorie refeeding in adolescents with anorexia nervosa: a narrative review.Acta Gastroenterol Belg. 2024 Apr-Jun;87(2):287-293. doi: 10.51821/87.2.12851. Acta Gastroenterol Belg. 2024. PMID: 39210761 Review.
Cited by
-
Clinical Outcomes of Refeeding Syndrome: A Systematic Review of High vs. Low-Calorie Diets for the Treatment of Anorexia Nervosa and Related Eating Disorders in Children and Adolescents.Cureus. 2023 May 21;15(5):e39313. doi: 10.7759/cureus.39313. eCollection 2023 May. Cureus. 2023. PMID: 37351245 Free PMC article. Review.
-
A prospective observational study examining weight and psychosocial change in adolescent and adult eating disorder inpatients admitted for nutritional rehabilitation using a high-energy re-feeding protocol.J Eat Disord. 2024 May 14;12(1):58. doi: 10.1186/s40337-024-01015-x. J Eat Disord. 2024. PMID: 38745266 Free PMC article.
-
Medical instability in typical and atypical adolescent anorexia nervosa: a systematic review and meta-analysis.J Eat Disord. 2023 Apr 6;11(1):58. doi: 10.1186/s40337-023-00779-y. J Eat Disord. 2023. PMID: 37024943 Free PMC article. Review.
-
Advancements in Inpatient Medical Management of Malnutrition in Children and Adolescents with Restrictive Eating Disorders.J Pediatr. 2023 Sep;260:113482. doi: 10.1016/j.jpeds.2023.113482. Epub 2023 May 15. J Pediatr. 2023. PMID: 37196778 Free PMC article.
-
The Diagnosis and Treatment of Anorexia Nervosa in Childhood and Adolescence.Dtsch Arztebl Int. 2024 Mar 8;121(5):164-174. doi: 10.3238/arztebl.m2023.0248. Dtsch Arztebl Int. 2024. PMID: 38170843 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
