

Use of Hyperoncotic Human Albumin Solution in Severe Traumatic Brain Injury Revisited-A Narrative Review and Meta-Analysis
- PMID: 35566786
- PMCID: PMC9099946
- DOI: 10.3390/jcm11092662
Use of Hyperoncotic Human Albumin Solution in Severe Traumatic Brain Injury Revisited-A Narrative Review and Meta-Analysis
Abstract
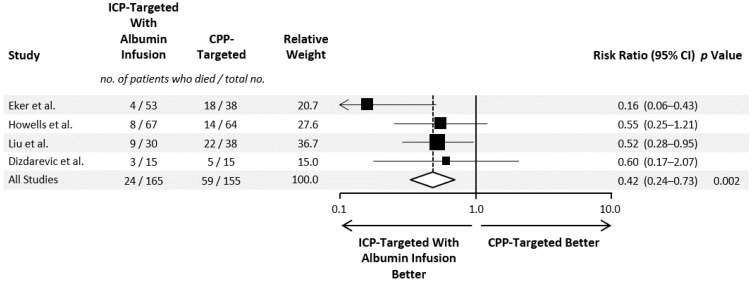
A significant proportion of patients with a severe traumatic brain injury (TBI) have hypoalbuminemia and require fluid resuscitation. Intravenous fluids can have both favorable and unfavorable consequences because of the risk of hyperhydration and hypo- or hyperosmolar conditions, which may affect the outcome of a TBI. Fluid resuscitation with human albumin solution (HAS) corrects low serum albumin levels and aids in preserving euvolemia in non-brain-injured intensive care units and in perioperative patients. However, the use of HAS for TBI remains controversial. In patients with TBI, the infusion of hypooncotic (4%) HAS was associated with adverse outcomes. The side effects of 4% HAS and the safety and efficacy of hyperoncotic (20-25%) HAS used in the Lund concept of TBI treatment need further investigation. A nonsystematic review, including a meta-analysis of controlled clinical trials, was performed to evaluate hyperoncotic HAS in TBI treatment. For the meta-analysis, the MEDLINE and EMBASE Library databases, as well as journal contents and reference lists, were searched for pertinent articles up to March 2021. Four controlled clinical studies involving 320 patients were included. The first was a randomized trial. Among 165 patients treated with hyperoncotic HAS, according to the Lund concept, 24 (14.5%) died vs. 59 out of 155 control patients (38.1%). A Lund concept intervention using hyperoncotic HAS was associated with a significantly reduced mortality (p = 0.002). Evidence of the beneficial effects of fluid management with hyperoncotic HAS on mortality in patients with TBI is at a high risk of bias. Prospective randomized controlled trials are required, which could lead to changes in clinical practice recommendations for fluid management in patients with TBI.
Keywords: albumin; brain injury; intracranial pressure; oncotic pressure; resuscitation.
Conflict of interest statement
C.J.W. received fees for speaking and/or consulting from CSL Behring and Biotest.
Figures
Similar articles
-
Albumin in Normovolemic Fluid Management for Severe Traumatic Brain Injury: Controversies and Research Gaps.J Clin Med. 2024 Sep 13;13(18):5452. doi: 10.3390/jcm13185452. J Clin Med. 2024. PMID: 39336939 Free PMC article.
-
The efficacy, safety and effectiveness of hyperoncotic albumin solutions in patients with sepsis: A systematic review and meta-analysis.J Intensive Care Soc. 2024 Jun 19;25(3):308-318. doi: 10.1177/17511437241259437. eCollection 2024 Aug. J Intensive Care Soc. 2024. PMID: 39224427 Free PMC article.
-
Phases of fluid management and the roles of human albumin solution in perioperative and critically ill patients.Curr Med Res Opin. 2020 Dec;36(12):1961-1973. doi: 10.1080/03007995.2020.1840970. Epub 2020 Nov 5. Curr Med Res Opin. 2020. PMID: 33090028 Review.
-
The evidence for small-volume resuscitation with hyperoncotic albumin in critical illness.Crit Care. 2008;12(2):143. doi: 10.1186/cc6882. Epub 2008 Apr 30. Crit Care. 2008. PMID: 18492216 Free PMC article.
-
Therapeutic effect of erythropoietin in patients with traumatic brain injury: a meta-analysis of randomized controlled trials.J Neurosurg. 2017 Jul;127(1):8-15. doi: 10.3171/2016.4.JNS152909. Epub 2016 Jul 1. J Neurosurg. 2017. PMID: 27367243
Cited by
-
European Society of Intensive Care Medicine clinical practice guideline on fluid therapy in adult critically ill patients. Part 1: the choice of resuscitation fluids.Intensive Care Med. 2024 Jun;50(6):813-831. doi: 10.1007/s00134-024-07369-9. Epub 2024 May 21. Intensive Care Med. 2024. PMID: 38771364
-
Albumin in Normovolemic Fluid Management for Severe Traumatic Brain Injury: Controversies and Research Gaps.J Clin Med. 2024 Sep 13;13(18):5452. doi: 10.3390/jcm13185452. J Clin Med. 2024. PMID: 39336939 Free PMC article.
-
Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years.J Clin Med. 2023 Sep 12;12(18):5919. doi: 10.3390/jcm12185919. J Clin Med. 2023. PMID: 37762860 Free PMC article. Review.
-
Prognosis and Clinical Significance of Piezo2 in Tumor: A Meta-analysis and Database Validation.Comb Chem High Throughput Screen. 2024;27(19):2912-2920. doi: 10.2174/0113862073251440231025111358. Comb Chem High Throughput Screen. 2024. PMID: 38347800
-
Fluid management strategies in critically ill patients with ARDS: a narrative review.Eur J Med Res. 2025 May 20;30(1):401. doi: 10.1186/s40001-025-02661-w. Eur J Med Res. 2025. PMID: 40394685 Free PMC article. Review.
References
-
- Juul N., Morris G.F., Marshall S.B., Marshall L.F. Intracranial Hypertension and Cerebral Perfusion Pressure: Influence on Neurological Deterioration and Outcome in Severe Head Injury. The Executive Committee of the International Selfotel Trial. J. Neurosurg. 2000;92:1–6. doi: 10.3171/jns.2000.92.1.0001. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
