

Bone marrow activation in response to metabolic syndrome and early atherosclerosis
- PMID: 35567559
- PMCID: PMC9113301
- DOI: 10.1093/eurheartj/ehac102
Bone marrow activation in response to metabolic syndrome and early atherosclerosis
Abstract
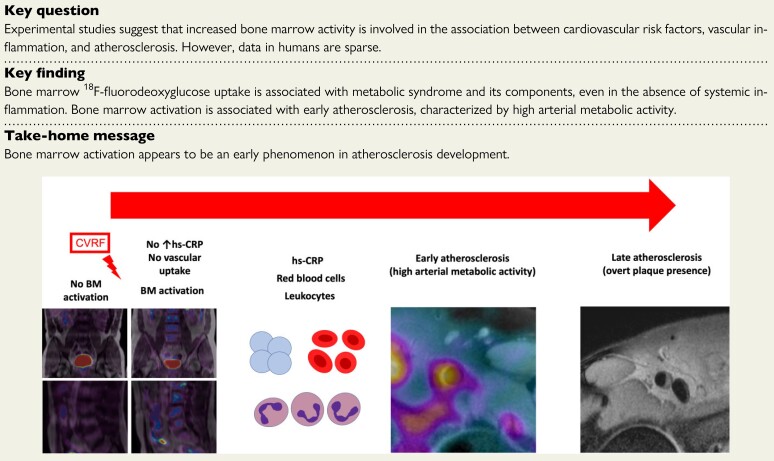
Aims: Experimental studies suggest that increased bone marrow (BM) activity is involved in the association between cardiovascular risk factors and inflammation in atherosclerosis. However, human data to support this association are sparse. The purpose was to study the association between cardiovascular risk factors, BM activation, and subclinical atherosclerosis.
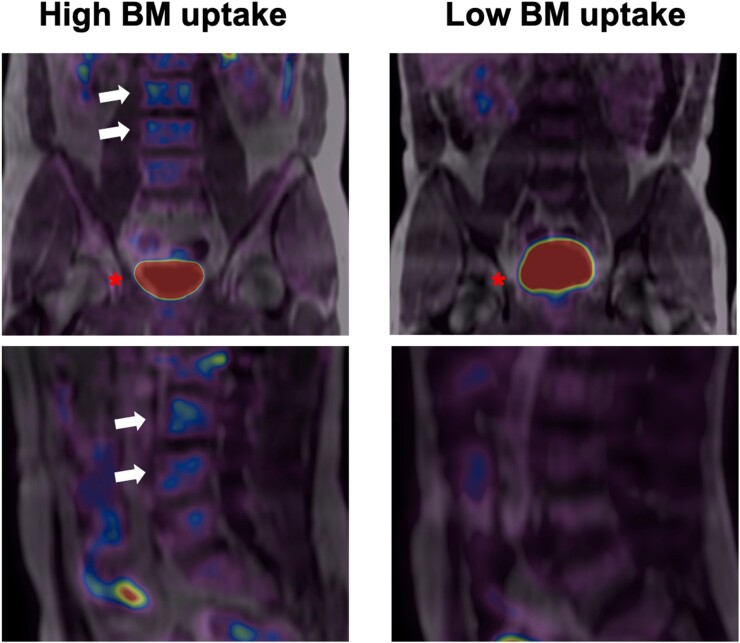
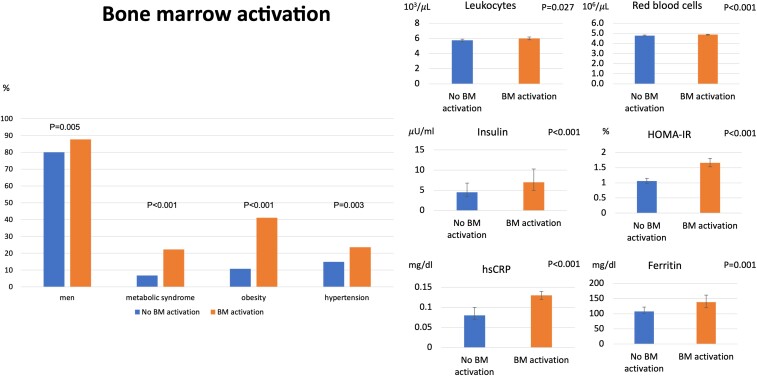
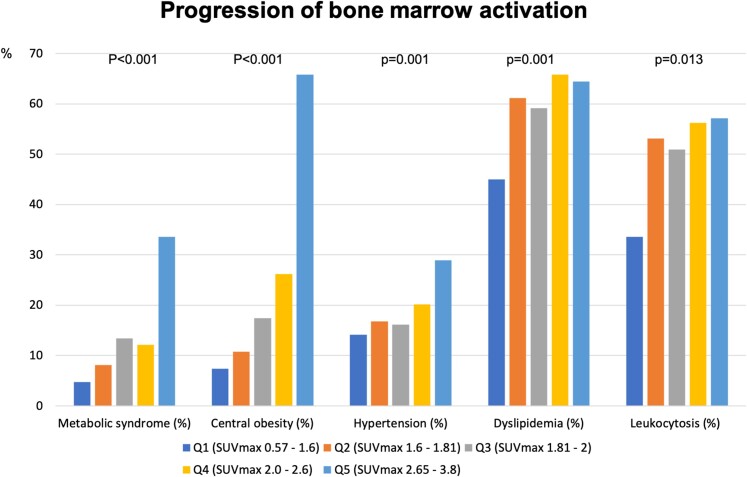
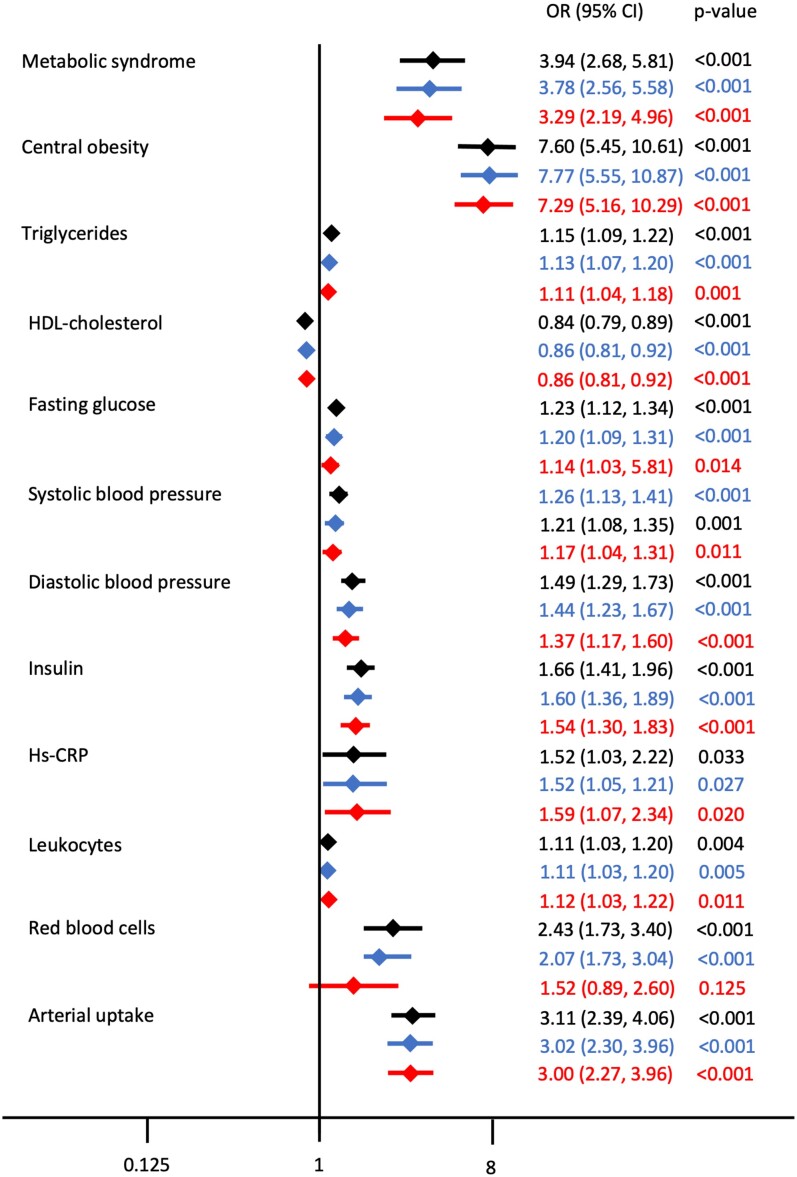
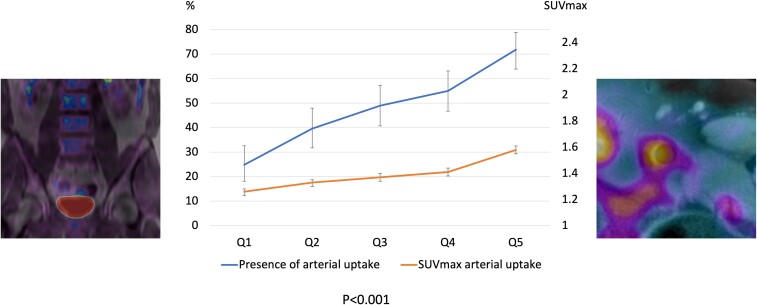
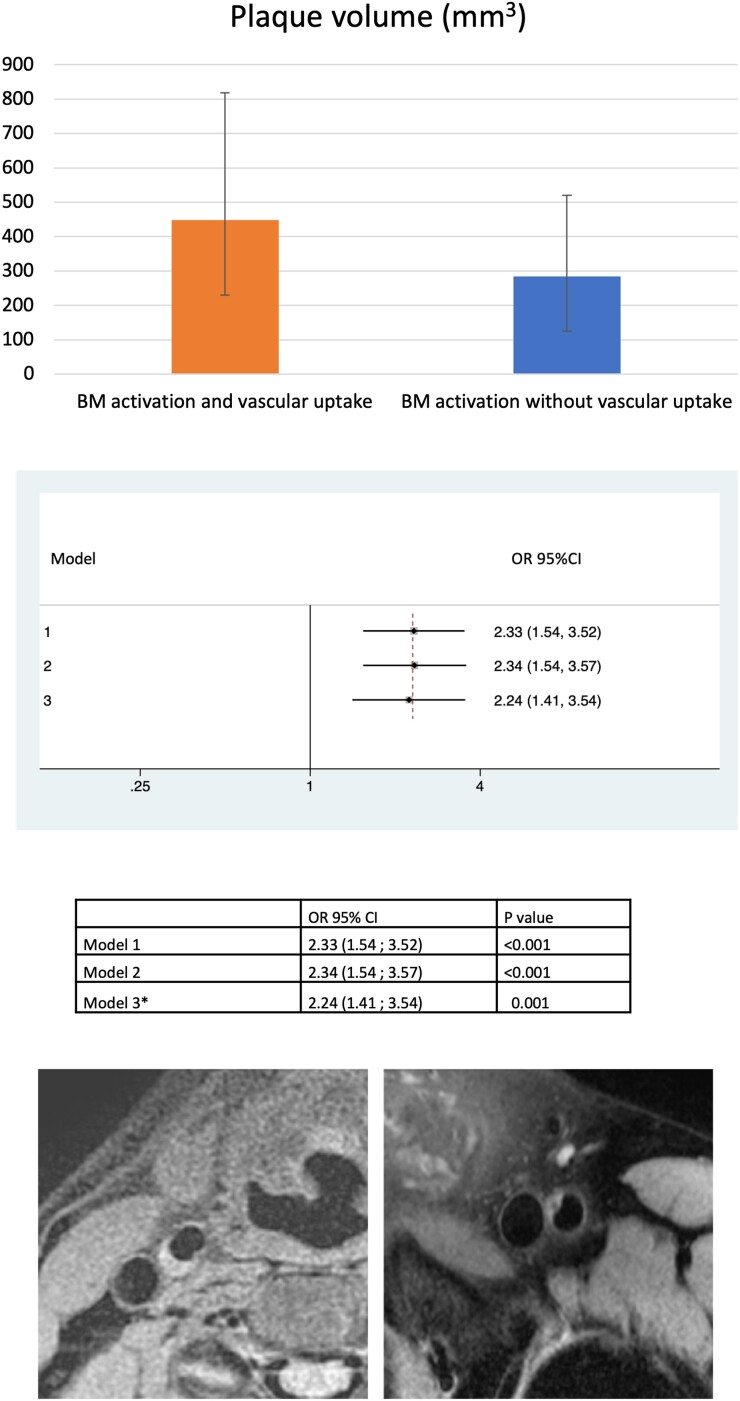
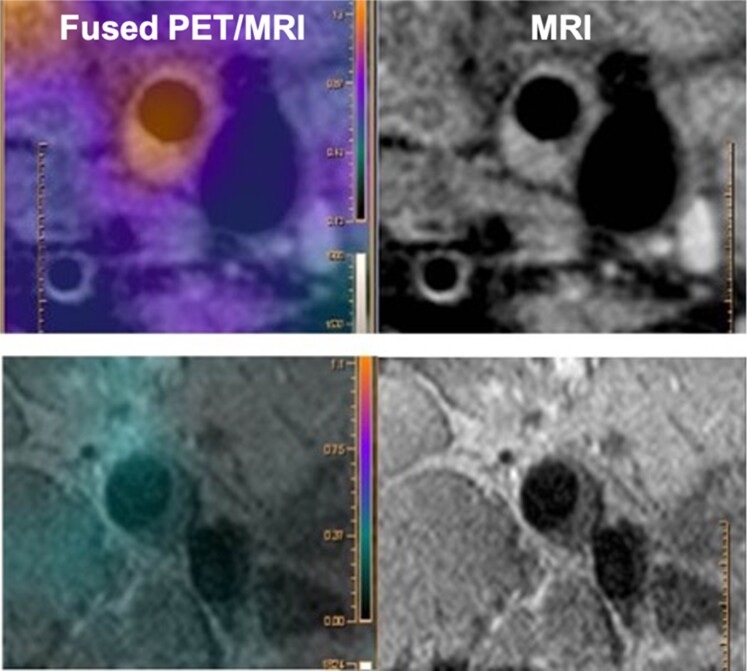
Methods and results: Whole body vascular 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging (18F-FDG PET/MRI) was performed in 745 apparently healthy individuals [median age 50.5 (46.8-53.6) years, 83.8% men] from the Progression of Early Subclinical Atherosclerosis (PESA) study. Bone marrow activation (defined as BM 18F-FDG uptake above the median maximal standardized uptake value) was assessed in the lumbar vertebrae (L3-L4). Systemic inflammation was indexed from circulating biomarkers. Early atherosclerosis was evaluated by arterial metabolic activity by 18F-FDG uptake in five vascular territories. Late atherosclerosis was evaluated by fully formed plaques on MRI. Subjects with BM activation were more frequently men (87.6 vs. 80.0%, P = 0.005) and more frequently had metabolic syndrome (MetS) (22.2 vs. 6.7%, P < 0.001). Bone marrow activation was significantly associated with all MetS components. Bone marrow activation was also associated with increased haematopoiesis-characterized by significantly elevated leucocyte (mainly neutrophil and monocytes) and erythrocyte counts-and with markers of systemic inflammation including high-sensitivity C-reactive protein, ferritin, fibrinogen, P-selectin, and vascular cell adhesion molecule-1. The associations between BM activation and MetS (and its components) and increased erythropoiesis were maintained in the subgroup of participants with no systemic inflammation. Bone marrow activation was significantly associated with high arterial metabolic activity (18F-FDG uptake). The co-occurrence of BM activation and arterial 18F-FDG uptake was associated with more advanced atherosclerosis (i.e. plaque presence and burden).
Conclusion: In apparently healthy individuals, BM 18F-FDG uptake is associated with MetS and its components, even in the absence of systemic inflammation, and with elevated counts of circulating leucocytes. Bone marrow activation is associated with early atherosclerosis, characterized by high arterial metabolic activity. Bone marrow activation appears to be an early phenomenon in atherosclerosis development.[Progression of Early Subclinical Atherosclerosis (PESA); NCT01410318].
Keywords: Bone marrow; Metabolic syndrome; PET/MRI; Subclinical atherosclerosis.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures
Comment in
-
Mischief in the marrow: a root of cardiovascular evil.Eur Heart J. 2022 May 14;43(19):1829-1831. doi: 10.1093/eurheartj/ehac149. Eur Heart J. 2022. PMID: 35567561 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
