

Ductal Carcinoma in Situ: Molecular Changes Accompanying Disease Progression
- PMID: 35567670
- PMCID: PMC9135892
- DOI: 10.1007/s10911-022-09517-7
Ductal Carcinoma in Situ: Molecular Changes Accompanying Disease Progression
Abstract
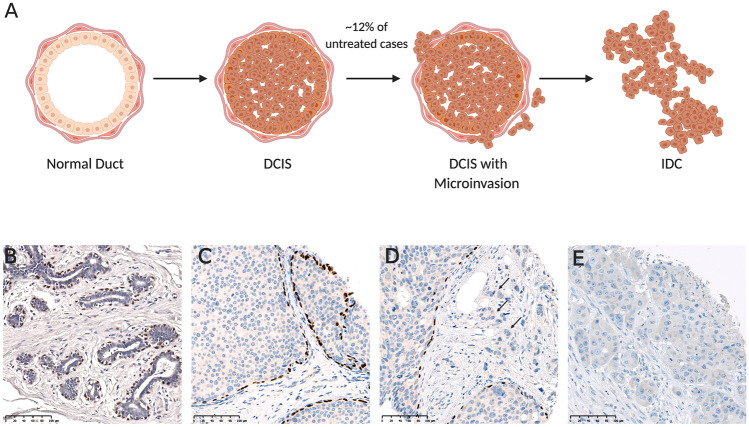
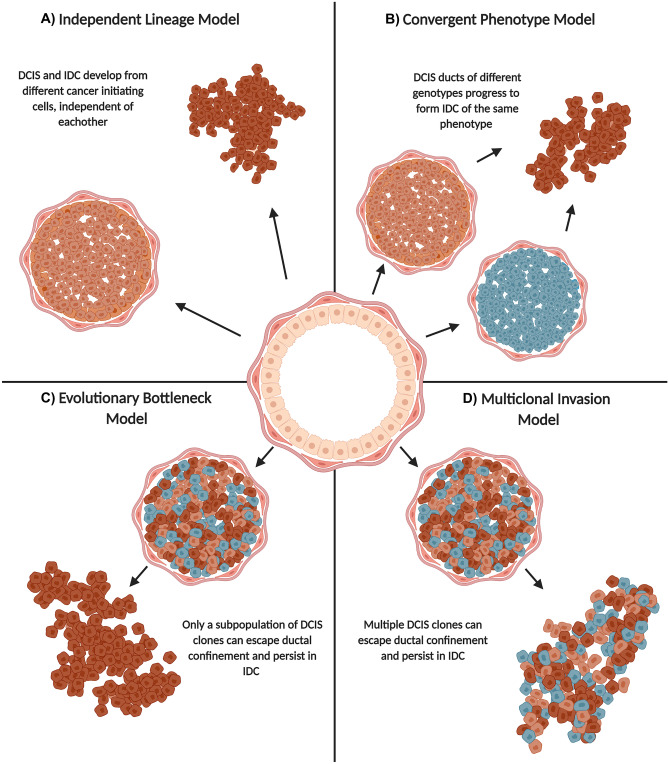
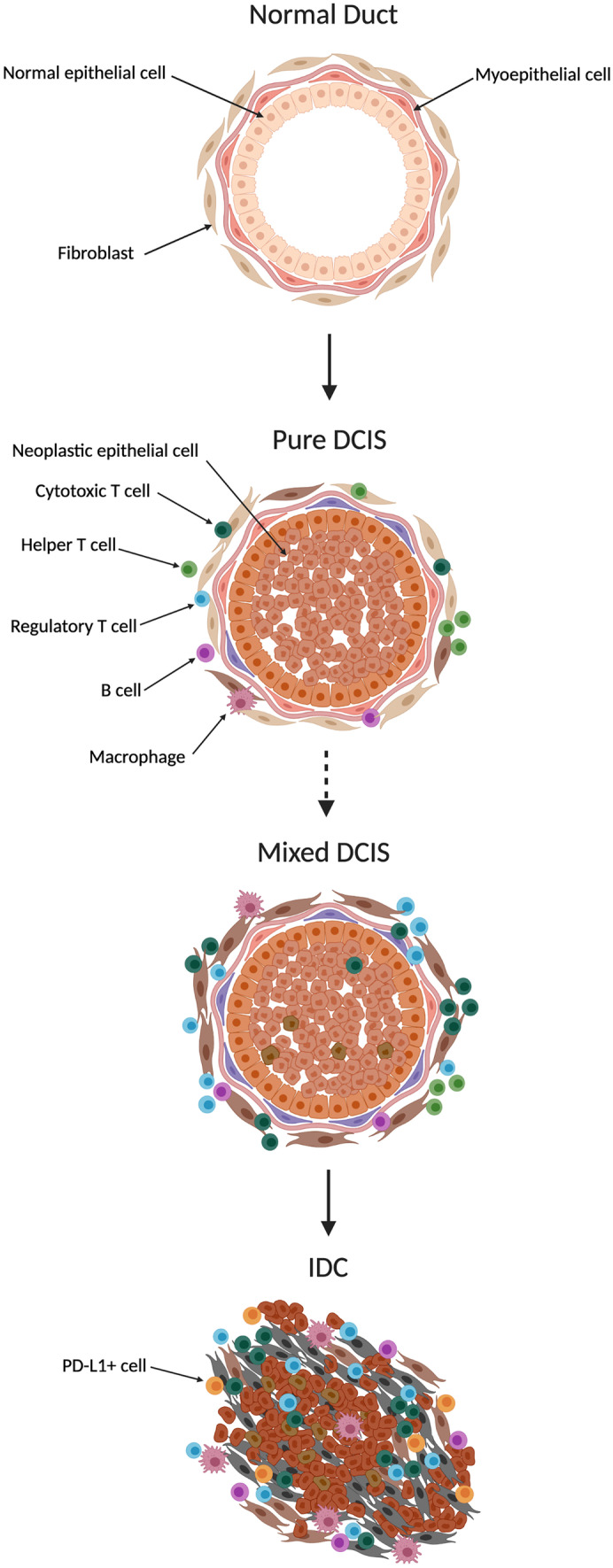
Ductal carcinoma in situ (DCIS) is a non-obligate precursor of invasive ductal carcinoma (IDC), whereby if left untreated, approximately 12% of patients develop invasive disease. The current standard of care is surgical removal of the lesion, to prevent potential progression, and radiotherapy to reduce risk of recurrence. There is substantial overtreatment of DCIS patients, considering not all DCIS lesions progress to invasive disease. Hence, there is a critical imperative to better predict which DCIS lesions are destined for poor outcome and which are not, allowing for tailored treatment. Active surveillance is currently being trialed as an alternative management practice, but this approach relies on accurately identifying cases that are at low risk of progression to invasive disease. Two DCIS-specific genomic profiling assays that attempt to distinguish low and high-risk patients have emerged, but imperfections in risk stratification coupled with a high price tag warrant the continued search for more robust and accessible prognostic biomarkers. This search has largely turned researchers toward the tumor microenvironment. Recent evidence suggests that a spectrum of cell types within the DCIS microenvironment are genetically and phenotypically altered compared to normal tissue and play critical roles in disease progression. Uncovering the molecular mechanisms contributing to DCIS progression has provided optimism for the search for well-validated prognostic biomarkers that can accurately predict the risk for a patient developing IDC. The discovery of such markers would modernize DCIS management and allow tailored treatment plans. This review will summarize the current literature regarding DCIS diagnosis, treatment, and pathology.
Keywords: Cancer progression; Ductal carcinoma in situ; Immune infiltration; Microenvironment.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Mariotti C. Ductal Carcinoma in Situ of the Breast. Cham: Springer International Publishing; 2018.
-
- Australian Institute of Health and Welfare . BreastScreen Australia monitoring report 2021. Canberra: AIHW; 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
