

Utility and pitfalls of the electrocardiogram in the evaluation of cardiac amyloidosis
- PMID: 35567784
- PMCID: PMC9296797
- DOI: 10.1111/anec.12967
Utility and pitfalls of the electrocardiogram in the evaluation of cardiac amyloidosis
Abstract
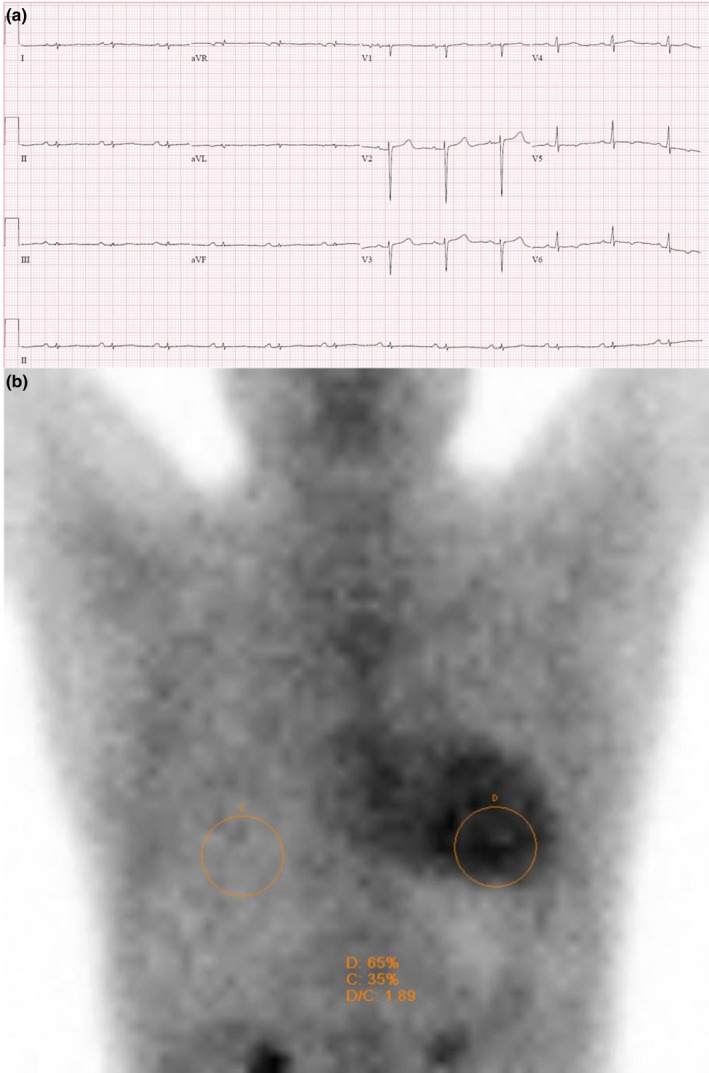
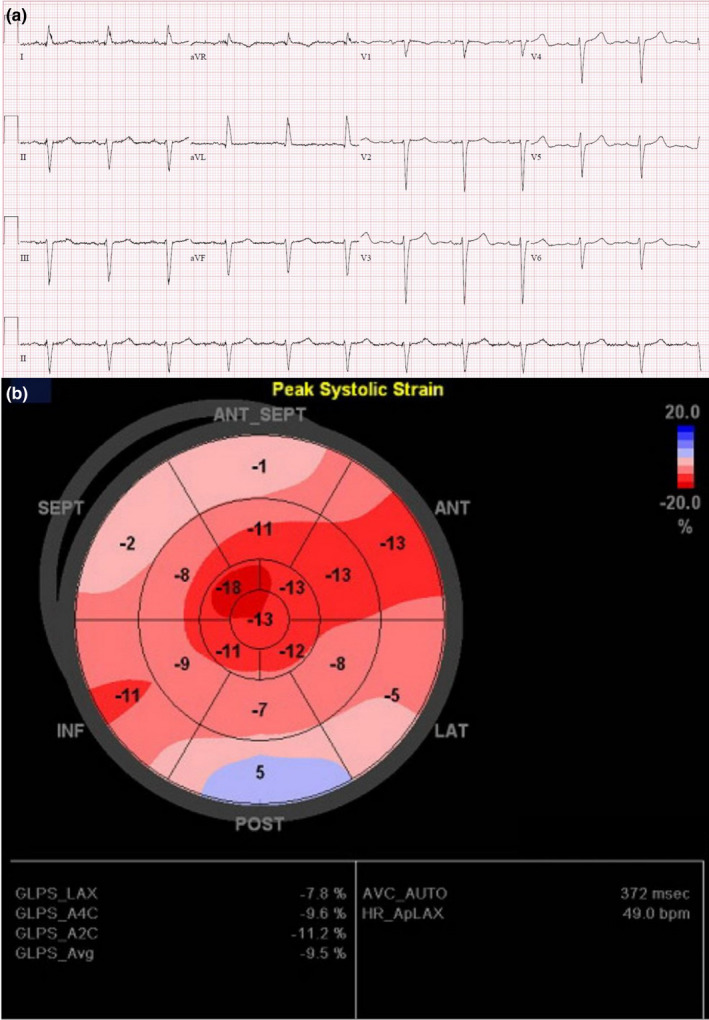
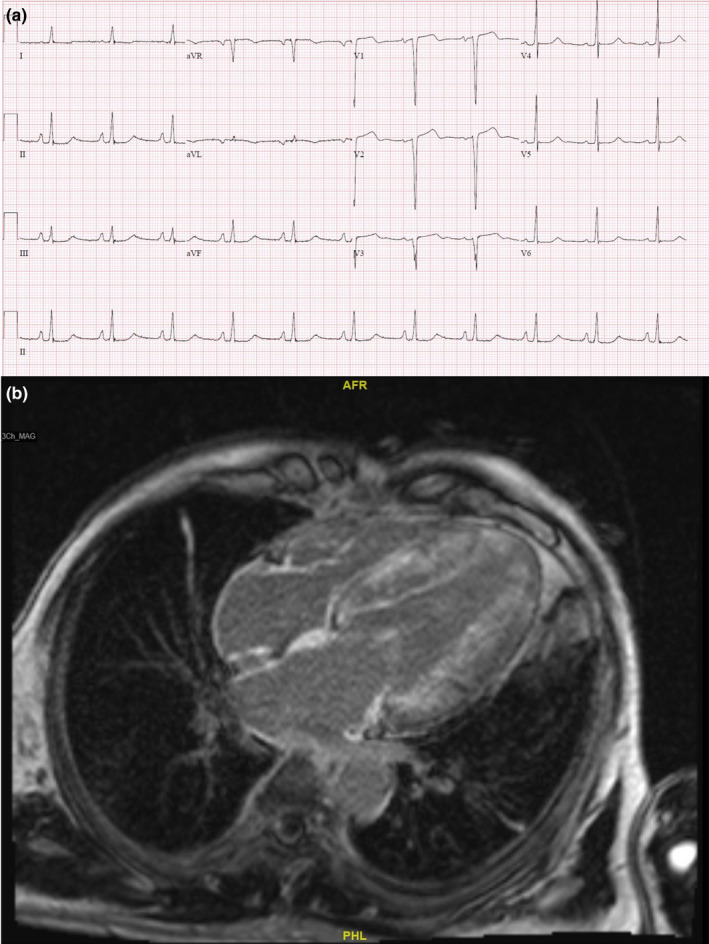
Background: Cardiac amyloidosis is a protein misfolding disorder involving deposition of amyloid fibril proteins in the heart. The associated fibrosis of the conduction tissue results in conduction abnormalities and arrhythmias. "Classical" electrocardiogram (ECG) findings in cardiac amyloidosis include that of low voltage complexes with increased left ventricular wall thickness on echocardiography. However, this "classical" finding is neither sensitive nor specific. As cardiac amyloidosis is associated with a generally poor prognosis, the need for early recognition of this disease is important given the availability of new treatment options. In this review, we highlight 3 cases of patients with cardiac amyloidosis. Although presenting with typical clinical signs and symptoms, ECG for all 3 patients was not consistent with the classical findings described. They underwent further diagnostic tests which clinched the diagnosis of cardiac amyloidosis, allowing patients to receive targeted treatment. Through the review of the literature, we will highlight the different ECG patterns in patients with different types of cardiac amyloidosis and clinical scenarios, as well as the pitfalls of using ECG to identify the condition. Lastly, we also emphasize the current paradigms in diagnosing cardiac amyloidosis through the non-invasive methods of echocardiography, cardiac magnetic resonance imaging, and nuclear technetium-pyrophosphate imaging.
Conclusions: Electrocardiogram is often the first investigation used in evaluating many cardiac disorders, including cardiac amyloidosis. However, classical features of cardiac amyloidosis on ECG are often not present. A keen understanding on the ECG features of cardiac amyloidosis and knowledge of the diagnostic workflow is important to diagnose this condition.
Keywords: cardiac amyloidosis; electrocardiogram; light chain amyloidosis; transthyretin amyloidosis.
© 2022 The Authors. Annals of Noninvasive Electrocardiology published by Wiley Periodicals LLC.
Conflict of interest statement
There is no conflict of interest for all authors.
Figures
References
-
- Bokhari, S. , Castaño, A. , Pozniakoff, T. , Deslisle, S. , Latif, F. , & Maurer, M. S. (2013). (99m)Tc‐pyrophosphate scintigraphy for differentiating light‐chain cardiac amyloidosis from the transthyretin‐related familial and senile cardiac amyloidoses. Circulation. Cardiovascular Imaging, 6, 195–201. - PMC - PubMed
-
- Cappelli, F. , Vignini, E. , Martone, R. , Perlini, S. , Mussinelli, R. , Sabena, A. , Morini, S. , Gabriele, M. , Taborchi, G. , Bartolini, S. , Lossi, A. , Nardi, G. , Marchionni, N. , di Mario, C. , Olivotto, I. , & Perfetto, F. (2020). Baseline ECG features and arrhythmic profile in transthyretin versus light chain cardiac amyloidosis. Circulation. Heart Failure, 13, e006619. - PubMed
-
- Carroll, J. D. , Gaasch, W. H. , & McAdam, K. P. (1982). Amyloid cardiomyopathy: Characterization by a distinctive voltage/mass relation. The American Journal of Cardiology, 49, 9–13. - PubMed
-
- Castano, A. , Narotsky, D. L. , Hamid, N. , Khalique, O. K. , Morgenstern, R. , DeLuca, A. , Rubin, J. , Chiuzan, C. , Nazif, T. , Vahl, T. , & George, I. (2017). Unveiling transthyretin cardiac amyloidosis and its predictors among elderly patients with severe aortic stenosis undergoing transcatheter aortic valve replacement. European Heart Journal, 38, 2879–2887. - PMC - PubMed
-
- Cavalcante, J. L. , Rijal, S. , Abdelkarim, I. , Althouse, A. D. , Sharbaugh, M. S. , Fridman, Y. , Soman, P. , Forman, D. E. , Schindler, J. T. , Gleason, T. G. , Lee, J. S. , & Schelbert, E. B. (2017). Cardiac amyloidosis is prevalent in older patients with aortic stenosis and carries worse prognosis. Journal of Cardiovascular Magnetic Resonance, 19, 98. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
