

Host and pathogen response to bacteriophage engineered against Mycobacterium abscessus lung infection
- PMID: 35568033
- PMCID: PMC9840467
- DOI: 10.1016/j.cell.2022.04.024
Host and pathogen response to bacteriophage engineered against Mycobacterium abscessus lung infection
Abstract
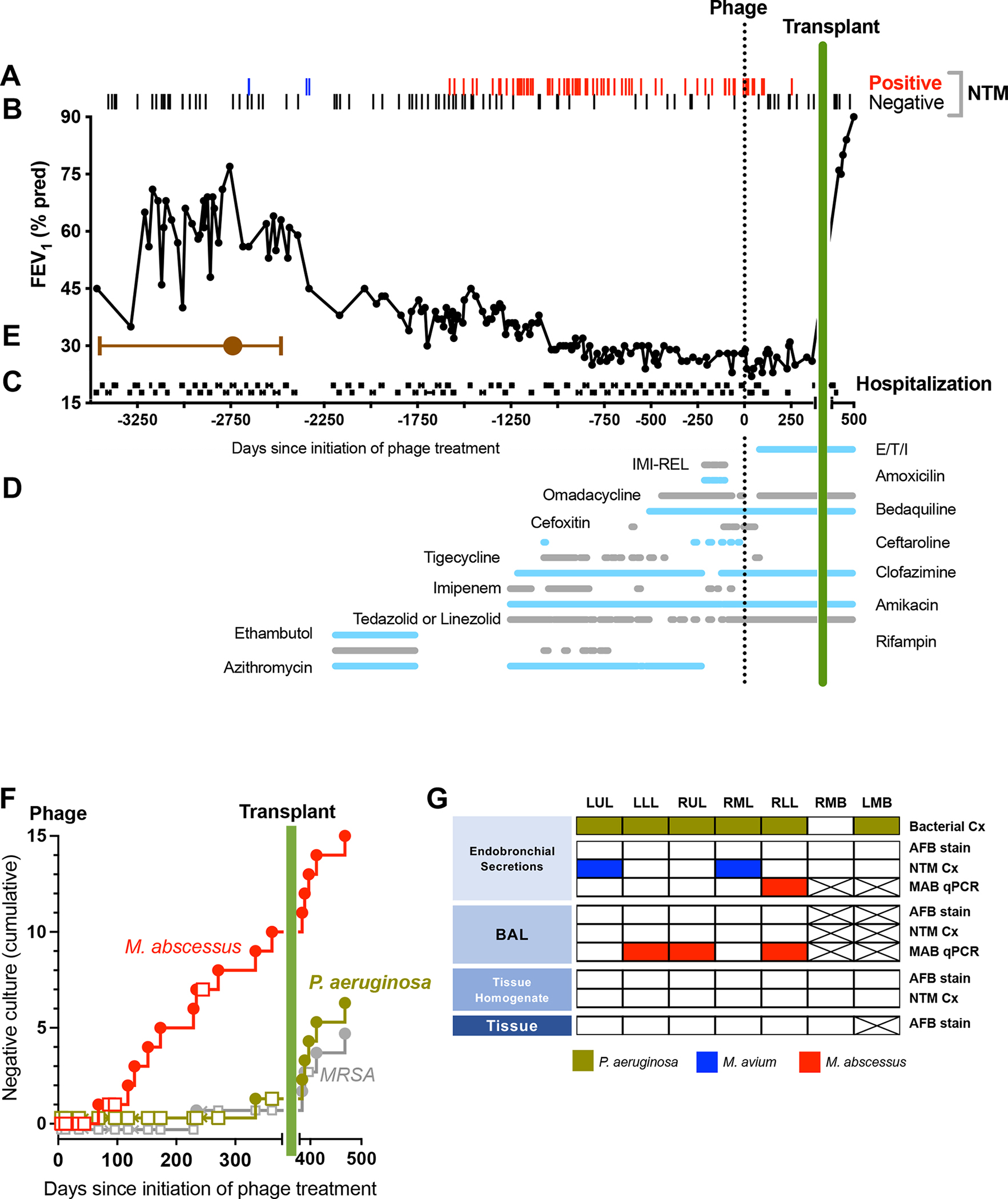
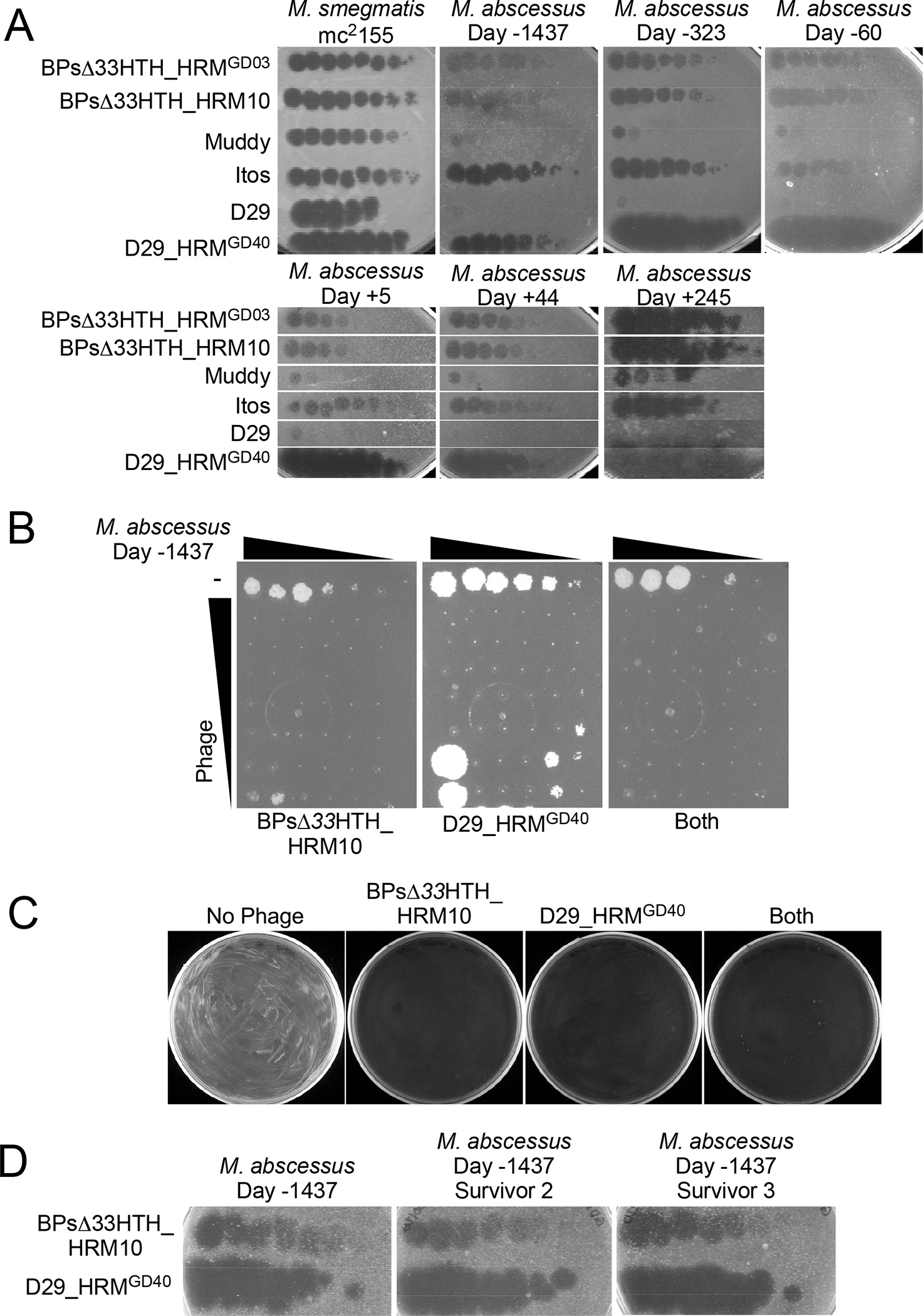
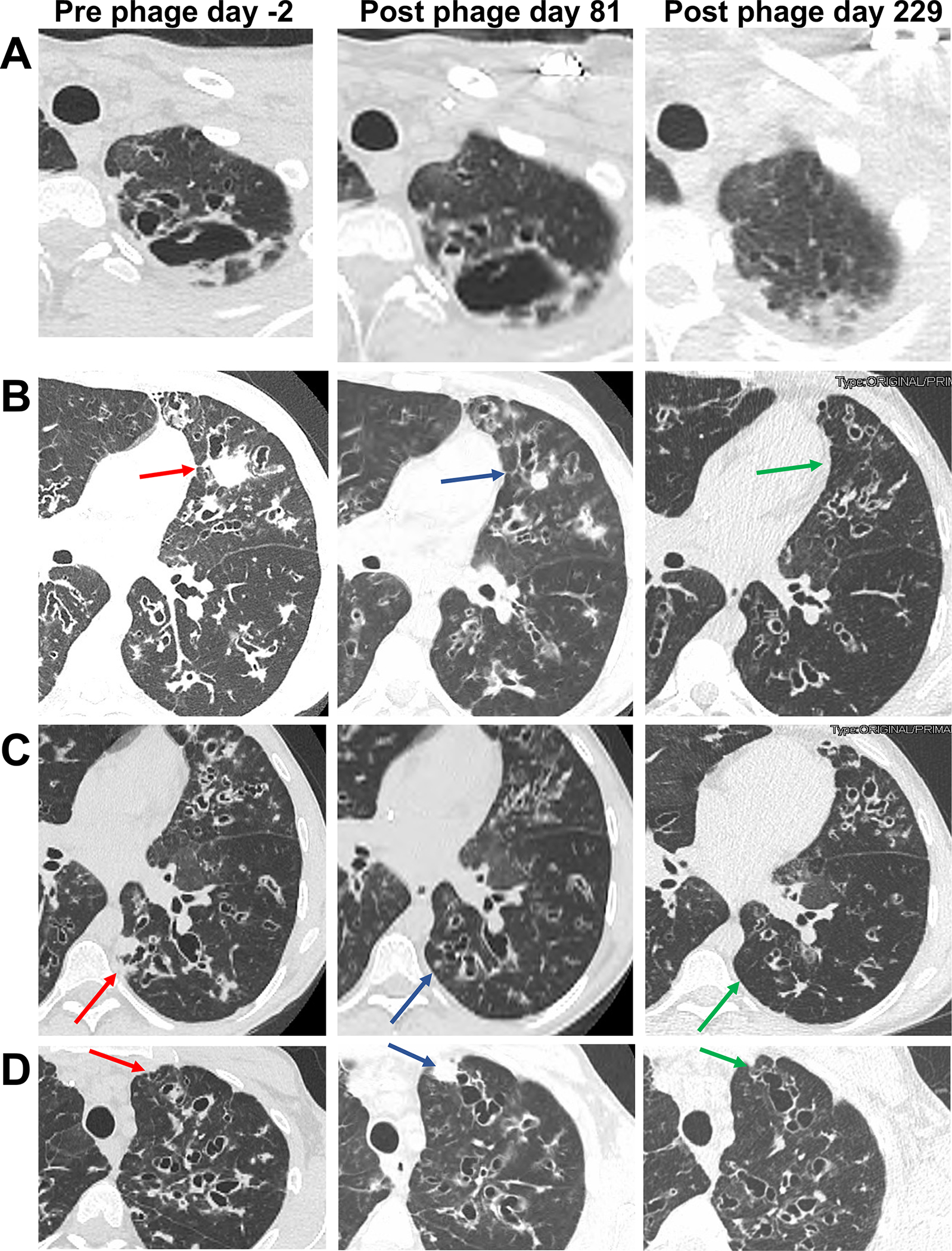
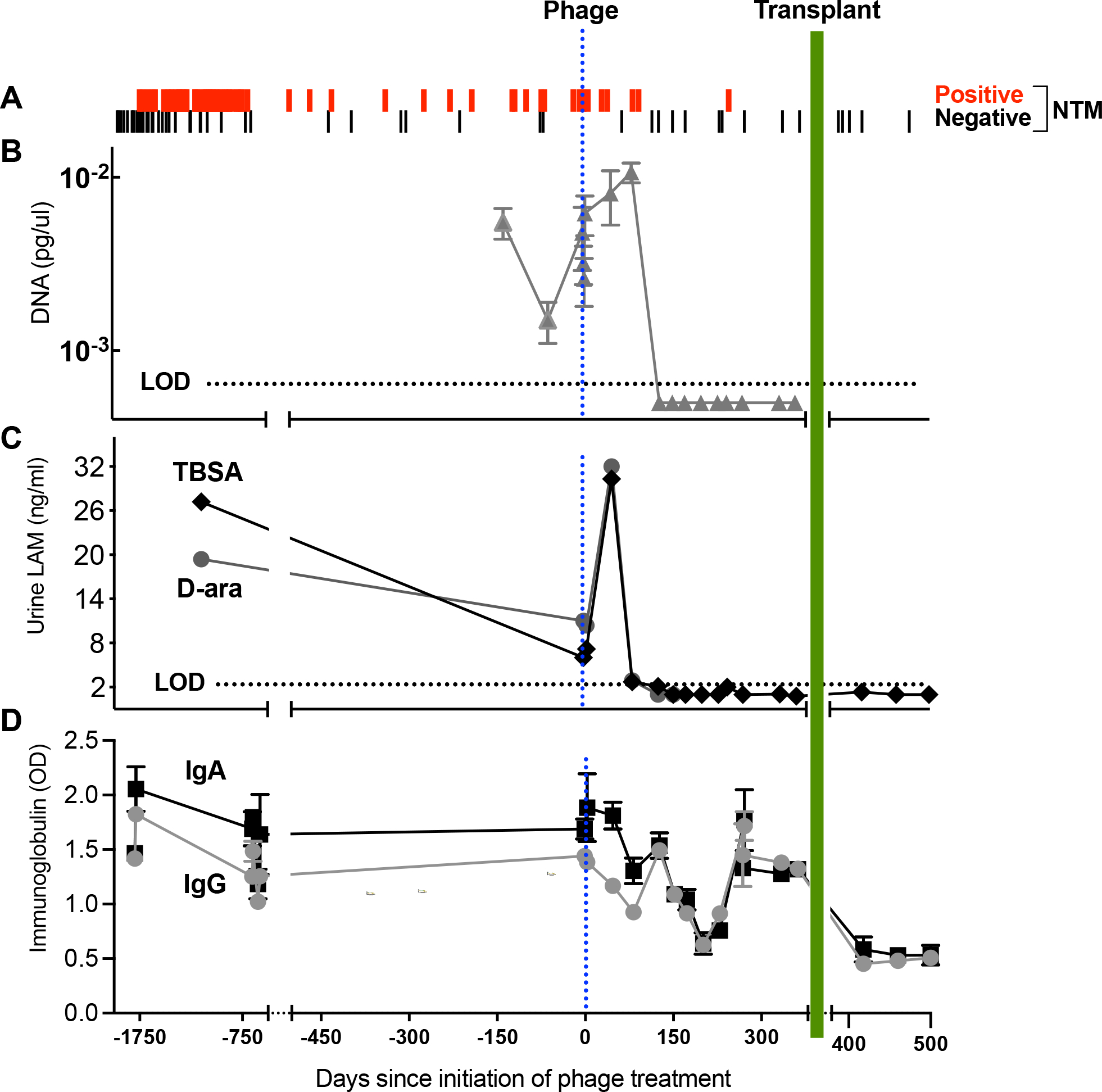
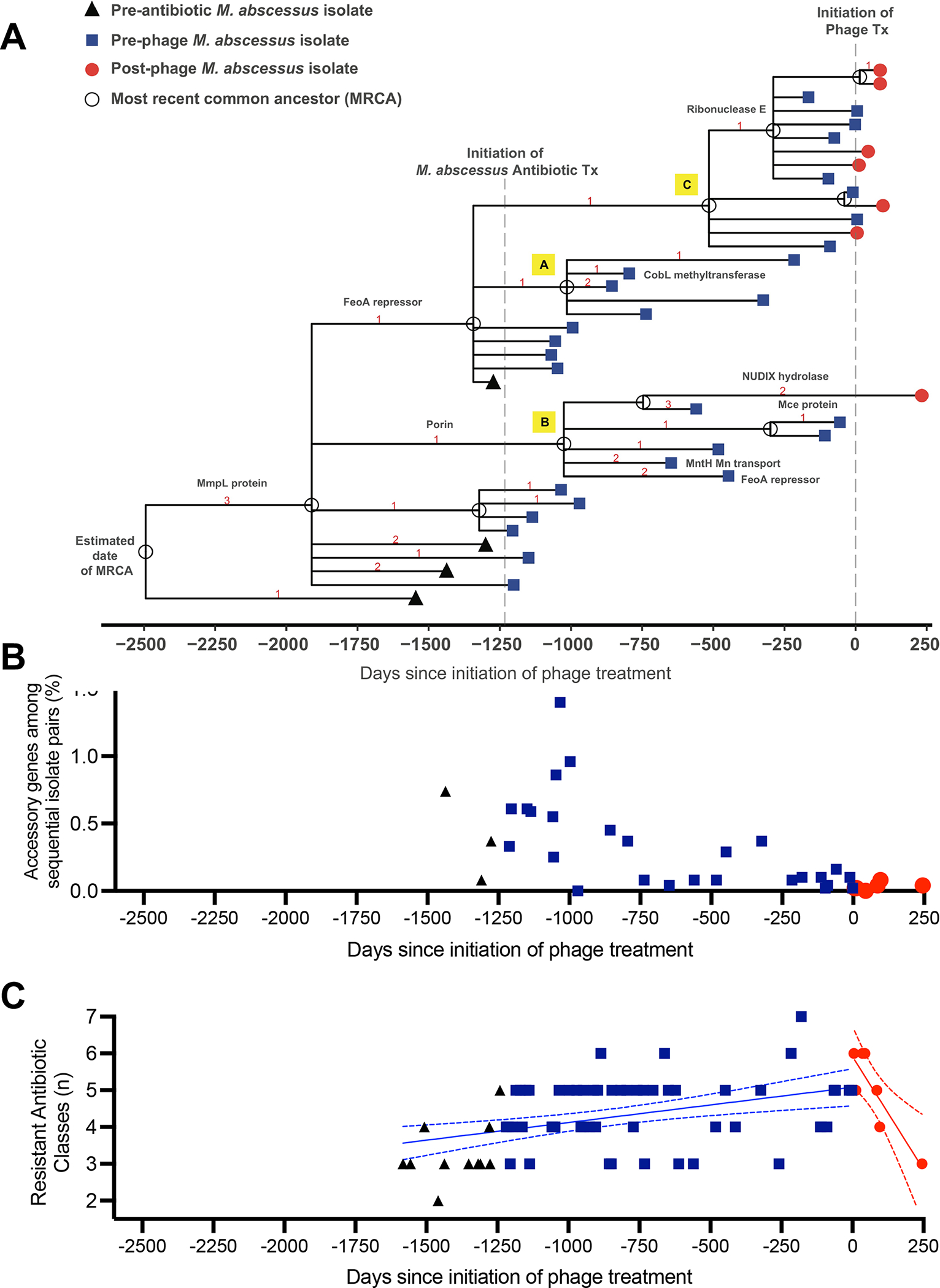
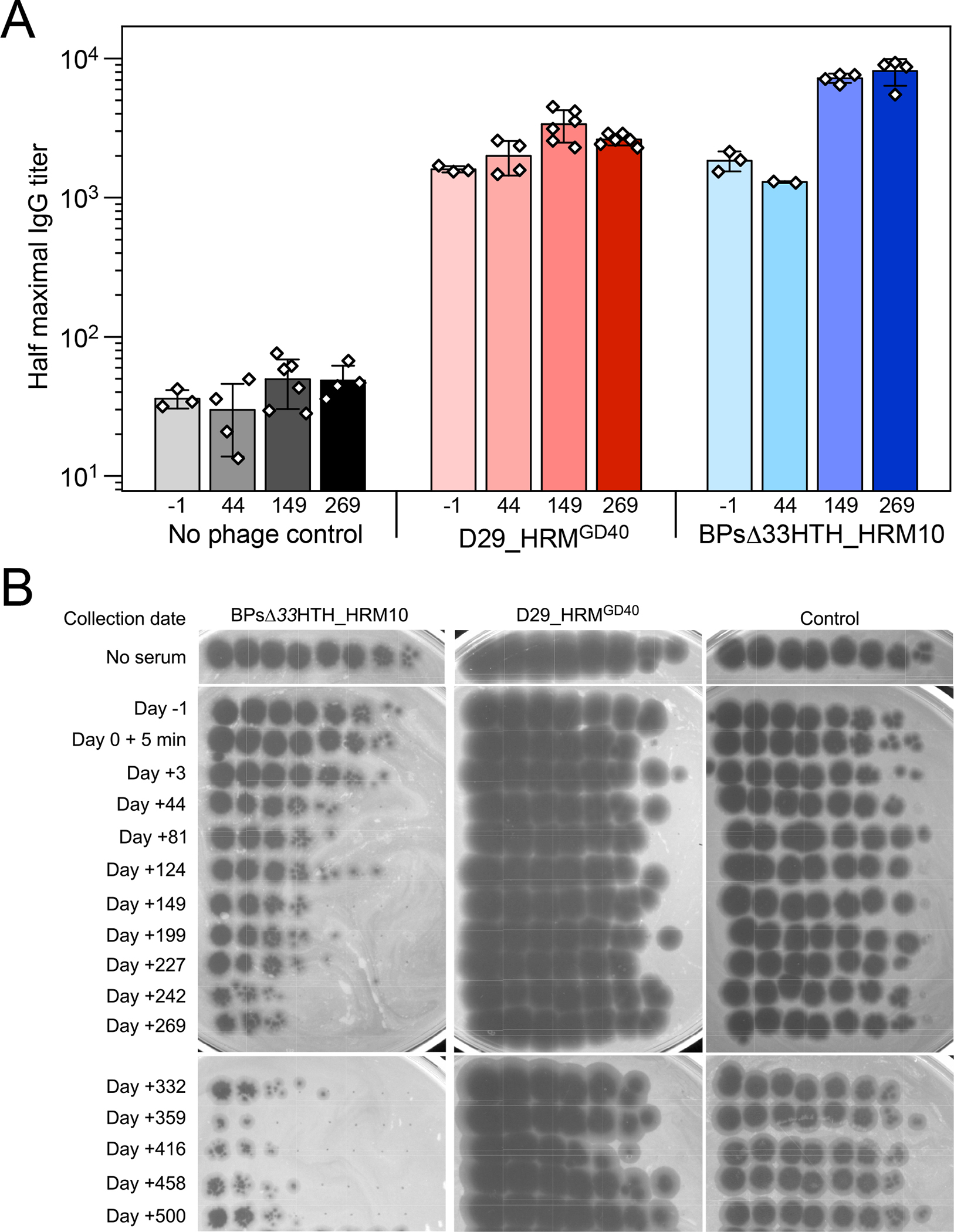
Two mycobacteriophages were administered intravenously to a male with treatment-refractory Mycobacterium abscessus pulmonary infection and severe cystic fibrosis lung disease. The phages were engineered to enhance their capacity to lyse M. abscessus and were selected specifically as the most effective against the subject's bacterial isolate. In the setting of compassionate use, the evidence of phage-induced lysis was observed using molecular and metabolic assays combined with clinical assessments. M. abscessus isolates pre and post-phage treatment demonstrated genetic stability, with a general decline in diversity and no increased resistance to phage or antibiotics. The anti-phage neutralizing antibody titers to one phage increased with time but did not prevent clinical improvement throughout the course of treatment. The subject received lung transplantation on day 379, and systematic culturing of the explanted lung did not detect M. abscessus. This study describes the course and associated markers of a successful phage treatment of M. abscessus in advanced lung disease.
Keywords: CFTR modulator therapy; Mycobacterium abscessus; Mycobacterium avium; NTM; bacteriophages; cystic fibrosis; immunoglobulin; lipoarabinomannan; lung transplant; nontuberculous mycobacterial lung disease.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests G.F.H. is a compensated consultant for Janssen Inc.
Figures
Comment in
-
Viruses to the rescue-Use of bacteriophage to treat resistant pulmonary infections.Cell. 2022 May 26;185(11):1807-1808. doi: 10.1016/j.cell.2022.04.037. Cell. 2022. PMID: 35623325
References
-
- Aslam S, Lampley E, Wooten D, Karris M, Benson C, Strathdee S, and Schooley RT (2020). Lessons Learned From the First 10 Consecutive Cases of Intravenous Bacteriophage Therapy to Treat Multidrug-Resistant Bacterial Infections at a Single Center in the United States. Open forum infectious diseases 7, ofaa389. - PMC - PubMed
-
- Champion OL, Karlyshev A, Cooper IAM, Ford DC, Wren BW, Duffield M, Oyston PCF, and Titball RW (2011). Yersinia pseudotuberculosis mntH functions in intracellular manganese accumulation, which is essential for virulence and survival in cells expressing functional Nramp1. Microbiology (Reading) 157, 1115–1122. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
