

Strategy to small intestine obstruction caused by Crohn's disease on the basis of transnasal ileus tube insertion
- PMID: 35568851
- PMCID: PMC9107679
- DOI: 10.1186/s12893-022-01632-w
Strategy to small intestine obstruction caused by Crohn's disease on the basis of transnasal ileus tube insertion
Abstract
Background: Previous studies reported that transnasal ileus tube was a new and useful method for rapid relief of small intestinal obstruction. However, no study reported the impacts of the transnasal ileus tube for Crohn's disease combined with intestinal obstruction. We aimed to describe the strategy to the small intestine obstruction caused by Crohn's disease on the basis of transnasal ileus tube insertion.
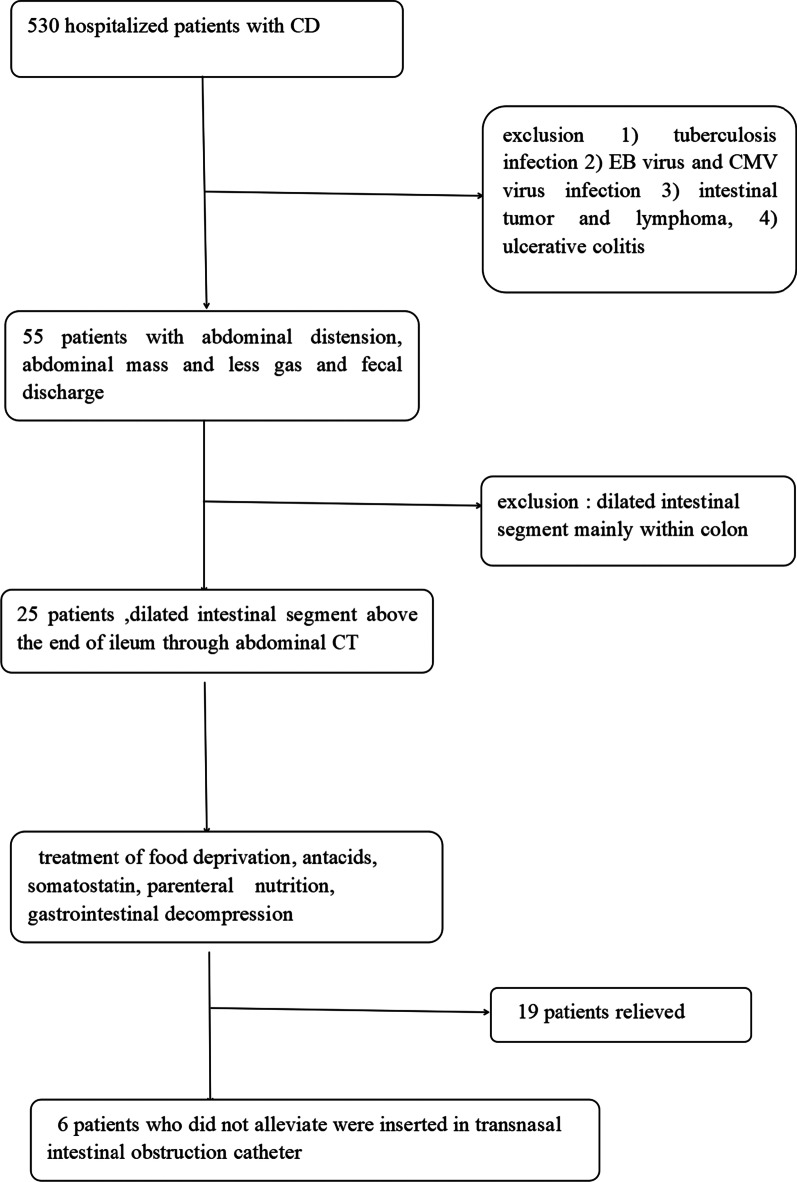
Methods: From November 2019 to November 2021, the data of 6 hospitalized patients with CD, diagnosed and conservatively treated in The Second Hospital of Nanjing, were not relived and retrospectively collected. After the insertion of transnasal ileus tube, demographic information, clinical features and treatment data were extracted from medical records.
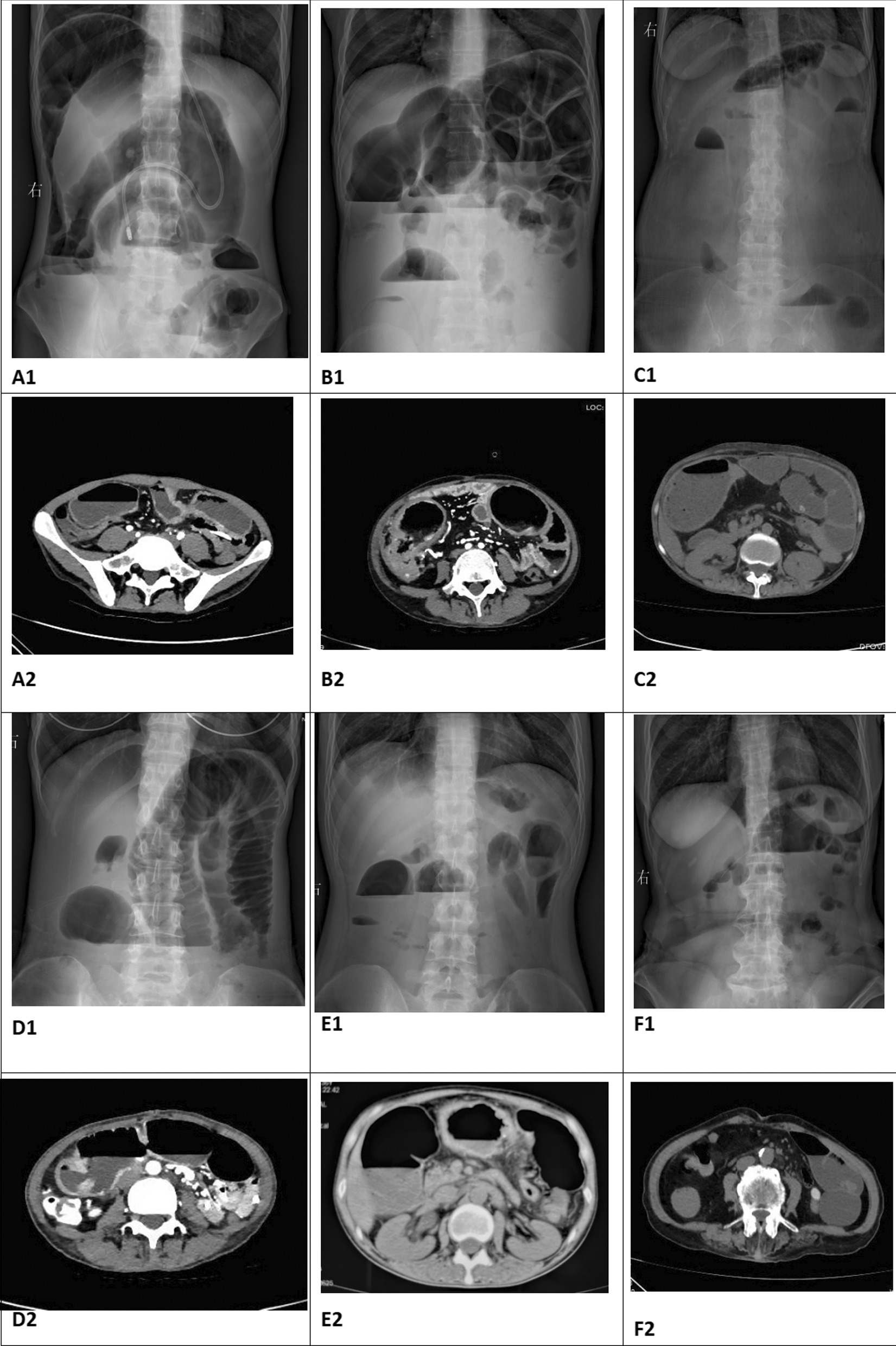
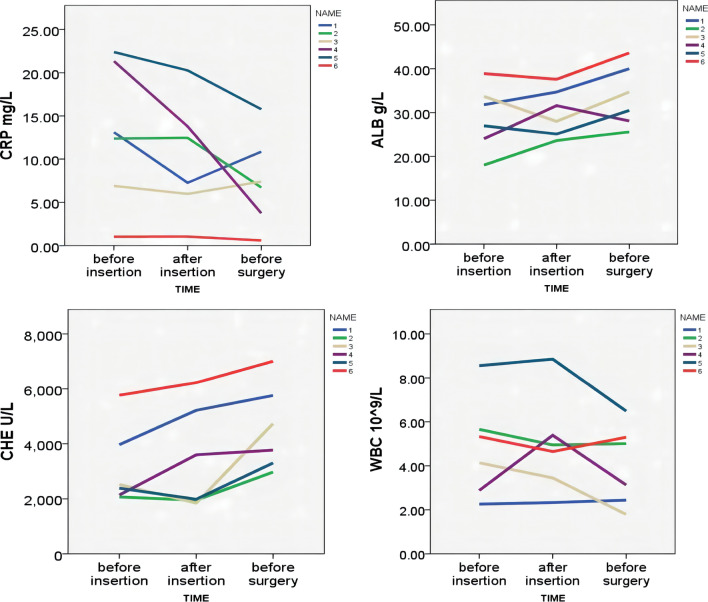
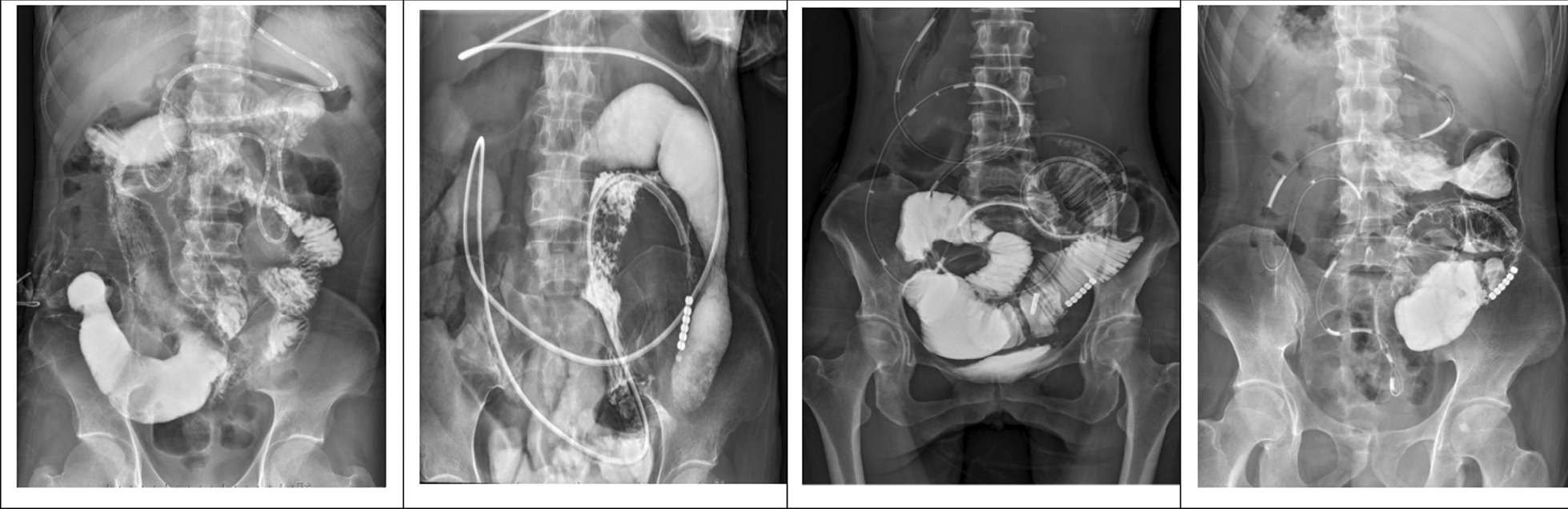
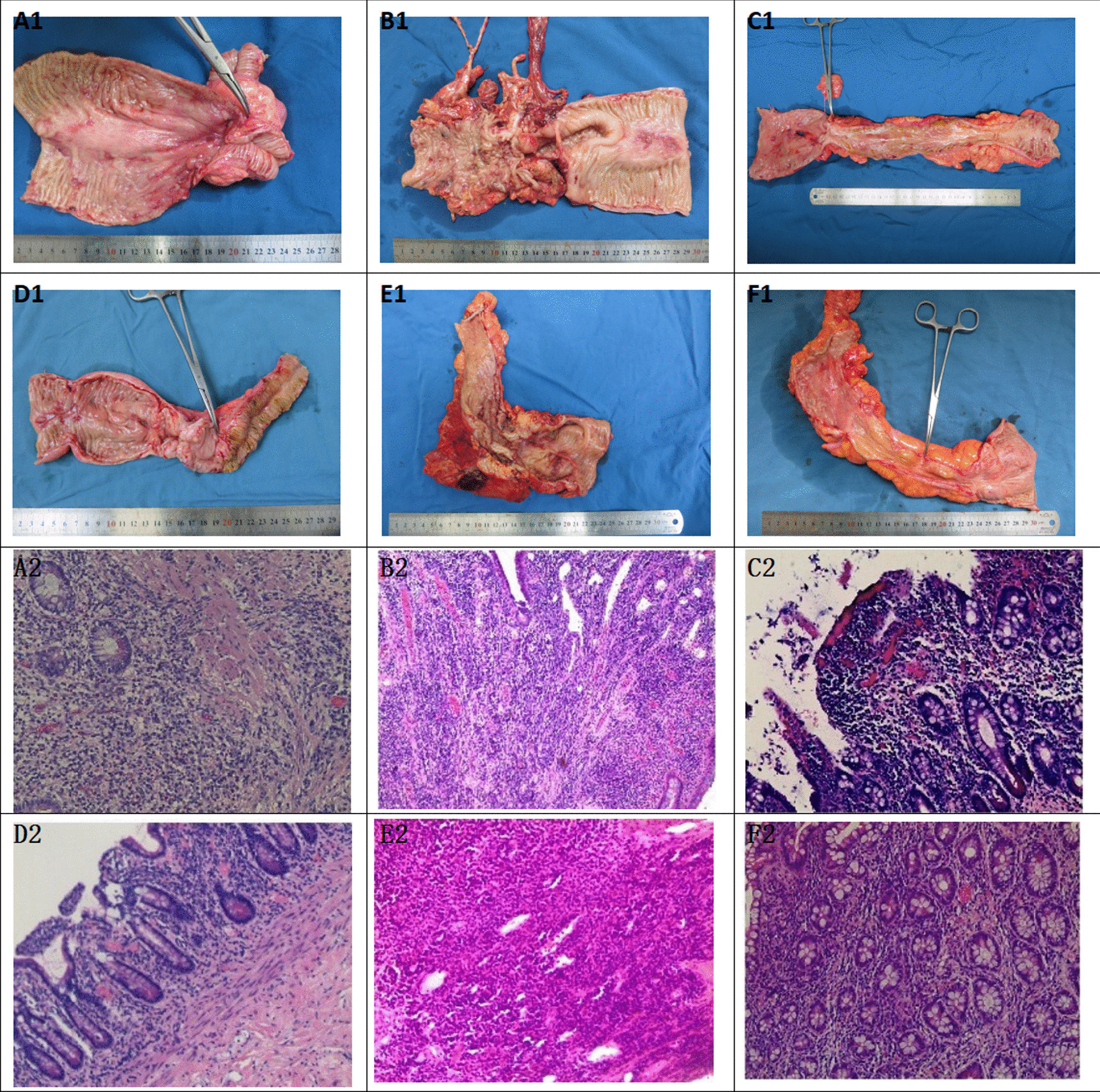
Results: Six Crohn's disease patients with intestinal obstruction were included. Half of them were male. The patients aged from 29 to 70 years. Five patients had chronic intestinal obstruction more than one year. Three patients had intestinal surgery history. One patient had colonic abdominal fistula and anastomotic fistula, when she took intermittent usage of sulfsalazine and steroid. On admission, all the patients had abdominal pain, distention and mass. Five patients had anemia, low albumin and cholinesterase. All CDAI scores were more than 400. Compared to 19 patients with incomplete intestinal obstruction improved by nasogastric decompression tube, 6 patients with intestinal obstruction catheter had significant difference in time for relieving abdominal pain and distension (p = 0.003), time for alleviating abnormal mass (p ≤ 0.01), drainage volume (p = 0.004), and preoperative CDAI score (p = 0.001). Compared with X-ray image before insertion, complete remission of obstruction of 5 patients were observed in intestinal cavity after insertion. After 1-2 months nutrition, all the patients had small intestine resection and ileostomy, half of them underwent colectomy and fistula repair, and 4 patients were performed enterolysis at the same time, the residual small intestine length ranging from 250 to 400 cm. 1 patient had permanent ileostomy;1 patient had abdominal infection after operation. The typical manifestations of acute and chronic inflammation, transmural inflammation, pseudopolyps and serous fiber hyperplasia could be seen in pathological findings of patients 1 to 5. All the patients continued enteral nutrition after surgery. Four patients were treated with infliximab or vedolizumab.
Conclusion: The current intestinal obstruction catheter which is used to treat patients with Crohn's combined obstruction can afford quick clinical remission, longer nutrition time, and suitable preoperative CDAI score for operation, which is worthy of wildly being used.
Keywords: Crohn’s disease; Obstructions; Transnasal ileus tube.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
Transanal ileus catheter combined with nasal ileus catheter in the treatment of malignant ileus in 14 cases: a case series and literature review.Ann Palliat Med. 2022 Nov;11(11):3520-3529. doi: 10.21037/apm-22-1233. Ann Palliat Med. 2022. PMID: 36464968 Review.
-
New insertion method of transnasal ileus tube for small bowel obstruction: Anterior balloon method.PLoS One. 2018 Nov 21;13(11):e0207099. doi: 10.1371/journal.pone.0207099. eCollection 2018. PLoS One. 2018. PMID: 30462677 Free PMC article.
-
Strictureplasty in Crohn's disease.Ann Surg. 1989 Nov;210(5):621-5. doi: 10.1097/00000658-198911000-00009. Ann Surg. 1989. PMID: 2818031 Free PMC article.
-
A prospective randomized trial of transnasal ileus tube vs nasogastric tube for adhesive small bowel obstruction.World J Gastroenterol. 2012 Apr 28;18(16):1968-74. doi: 10.3748/wjg.v18.i16.1968. World J Gastroenterol. 2012. PMID: 22563179 Free PMC article. Clinical Trial.
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
Cited by
-
Efficacy of ileus tube combined with meglumine diatrizoate in treating postoperative inflammatory bowel obstruction after surgery.World J Gastrointest Surg. 2023 Sep 27;15(9):1950-1958. doi: 10.4240/wjgs.v15.i9.1950. World J Gastrointest Surg. 2023. PMID: 37901727 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
