

Prediabetes and insulin resistance in a population of patients with heart failure and reduced or preserved ejection fraction but without diabetes, overweight or hypertension
- PMID: 35568879
- PMCID: PMC9107647
- DOI: 10.1186/s12933-022-01509-5
Prediabetes and insulin resistance in a population of patients with heart failure and reduced or preserved ejection fraction but without diabetes, overweight or hypertension
Abstract
Background: The relationships between glucose abnormalities, insulin resistance (IR) and heart failure (HF) are unclear, especially regarding to the HF type, i.e., HF with reduced (HFrEF) or preserved (HFpEF) ejection fraction. Overweight, diabetes and hypertension are potential contributors to IR in persons with HF. This study aimed to evaluate the prevalence of prediabetes and IR in a population of Vietnamese patients with HFrEF or HFpEF but no overweight, diabetes or hypertension, in comparison with healthy controls, and the relation between prediabetes or IR and HF severity.
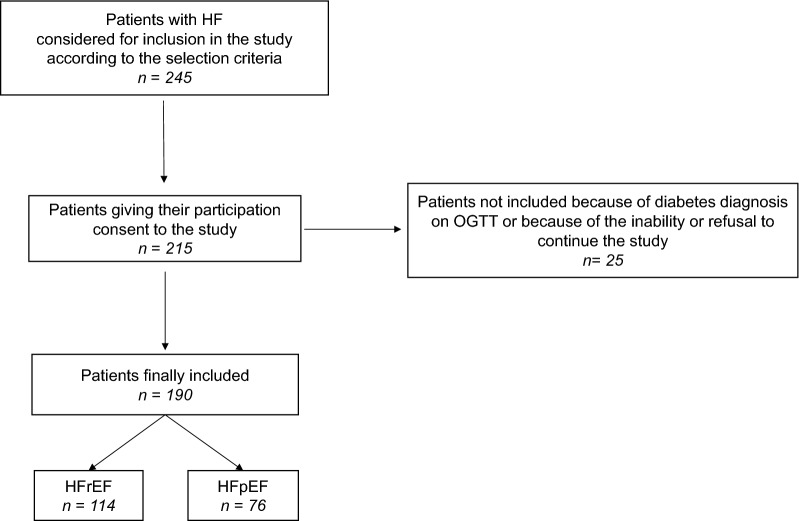
Methods: We conducted a prospective cross-sectional observational study in 190 non-overweight normotensive HF patients (114 with HFrEF and 76 with HFpEF, 92.6% were ischemic HF, mean age was 70.1 years, mean BMI 19.7 kg/m2) without diabetes (neither known diabetes nor newly diagnosed by OGTT) and 95 healthy individuals (controls). Prediabetes was defined using 2006 WHO criteria. Glucose and insulin levels were measured fasting and 2 h after glucose challenge. IR was assessed using HOMA-IR and several other indexes.
Results: Compared to controls, HF patients had a higher prevalence of prediabetes (63.2% vs 22.1%) and IR (according to HOMA-IR, 55.3% vs 26.3%), higher HOMA-IR, insulin/glucose ratio after glucose and FIRI, and lower ISIT0 and ISIT120 (< 0.0001 for all comparisons), with no difference for body weight, waist circumference, blood pressure and lipid parameters. Prediabetes was more prevalent (69.3% vs 53.9%, p = 0.03) and HOMA-IR was higher (p < 0.0001) in patients with HFrEF than with HFpEF. Among both HFrEF and HFpEF patients, those with prediabetes or IR had a more severe HF (higher NYHA functional class and NT-proBNP levels, lower ejection fraction; p = 0.04-< 0.0001) than their normoglycemic or non-insulinresistant counterparts, with no difference for blood pressure and lipid parameters.
Conclusion: In non-diabetic non-overweight normotensive patients with HF, the prevalence of prediabetes is higher with some trend to more severe IR in those with HFrEF than in those with HFpEF. Both prediabetes and IR are associated with a more severe HF. The present data support HF as a culprit for IR. Intervention strategies should be proposed to HF patients with prediabetes aiming to reduce the risk of incident diabetes. Studies should be designed to test whether such strategies may translate into an improvement of further HF-related outcomes.
Keywords: Heart failure; Heart failure with preserved ejection fraction; Heart failure with reduced ejection fraction; Insulin resistance; Oral glucose tolerance test; Prediabetes.
© 2022. The Author(s).
Conflict of interest statement
PV discloses the following potential conflicts of interest: lectures for Abbott, AstraZeneca, Bayer, Eli Lilly, Hikma Pharmaceuticals, Merck Sharp & Dohme, Novo Nordisk, Novartis, Pfizer, Sanofi; research grants from Abbott, Bristol-Myers Squibb–AstraZeneca, Novo Nordisk; participation in expert committees for AstraZeneca, Boehringer Ingelheim, Novo Nordisk, Daiichi Sankyo, Sanofi, Servier. The other authors declare they have no conflict of interest.
Similar articles
-
Insulin resistance in heart failure: differences between patients with reduced and preserved left ventricular ejection fraction.Eur J Heart Fail. 2015 Oct;17(10):1015-21. doi: 10.1002/ejhf.317. Epub 2015 Jul 21. Eur J Heart Fail. 2015. PMID: 26198713
-
Glycemic Markers and Heart Failure Subtypes: The Multi-Ethnic Study of Atherosclerosis (MESA).J Card Fail. 2022 Nov;28(11):1593-1603. doi: 10.1016/j.cardfail.2022.01.011. Epub 2022 Jan 31. J Card Fail. 2022. PMID: 35114382 Free PMC article.
-
Prevalence of Prediabetes and Undiagnosed Diabetes in Patients with HFpEF and HFrEF and Associated Clinical Outcomes.Cardiovasc Drugs Ther. 2017 Dec;31(5-6):545-549. doi: 10.1007/s10557-017-6754-x. Cardiovasc Drugs Ther. 2017. PMID: 28948430 Free PMC article.
-
Evidence of a bi-directional relationship between heart failure and diabetes: a strategy for the detection of glucose abnormalities and diabetes prevention in patients with heart failure.Cardiovasc Diabetol. 2024 Sep 28;23(1):354. doi: 10.1186/s12933-024-02436-3. Cardiovasc Diabetol. 2024. PMID: 39342254 Free PMC article. Review.
-
Diabetes mellitus and risk of new-onset and recurrent heart failure: a systematic review and meta-analysis.ESC Heart Fail. 2020 Oct;7(5):2146-2174. doi: 10.1002/ehf2.12782. Epub 2020 Jul 29. ESC Heart Fail. 2020. PMID: 32725969 Free PMC article.
Cited by
-
Usefulness of estimated glucose disposal rate in detecting heart failure: results from national health and nutrition examination survey 1999-2018.Diabetol Metab Syndr. 2024 Aug 5;16(1):189. doi: 10.1186/s13098-024-01402-z. Diabetol Metab Syndr. 2024. PMID: 39103949 Free PMC article.
-
Prognostic Implications of Insulin Resistance in Heart Failure in Japan.Nutrients. 2024 Jun 14;16(12):1888. doi: 10.3390/nu16121888. Nutrients. 2024. PMID: 38931242 Free PMC article.
-
Glucose-Induced Hemodynamic and Metabolic Response of Skeletal Muscle in Heart Failure Patients with Reduced vs. Preserved Ejection Fraction-A Pilot Study.J Cardiovasc Dev Dis. 2022 Dec 13;9(12):456. doi: 10.3390/jcdd9120456. J Cardiovasc Dev Dis. 2022. PMID: 36547453 Free PMC article.
-
In-Vitro and In-Silico Studies of Brevifoliol Ester Analogues against Insulin Resistance Condition.Curr Diabetes Rev. 2025;21(7):1-9. doi: 10.2174/0115733998275238240116083227. Curr Diabetes Rev. 2025. PMID: 39257150
-
Temporal prevalence and prognostic impact of diabetes mellitus and albuminuria in heart failure with preserved ejection fraction.Cardiovasc Diabetol. 2025 Apr 5;24(1):156. doi: 10.1186/s12933-025-02708-6. Cardiovasc Diabetol. 2025. PMID: 40188061 Free PMC article.
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Colvin MM, et al. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2017;136:e137–e161. doi: 10.1161/CIR.0000000000000509. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
