

Biomechanical study of oblique lumbar interbody fusion (OLIF) augmented with different types of instrumentation: a finite element analysis
- PMID: 35568923
- PMCID: PMC9107272
- DOI: 10.1186/s13018-022-03143-z
Biomechanical study of oblique lumbar interbody fusion (OLIF) augmented with different types of instrumentation: a finite element analysis
Abstract
Background: To explore the biomechanical differences in oblique lumbar interbody fusion (OLIF) augmented by different types of instrumentation.
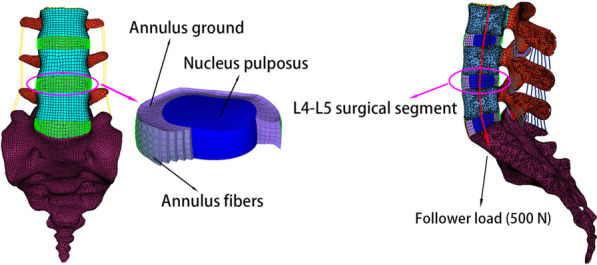
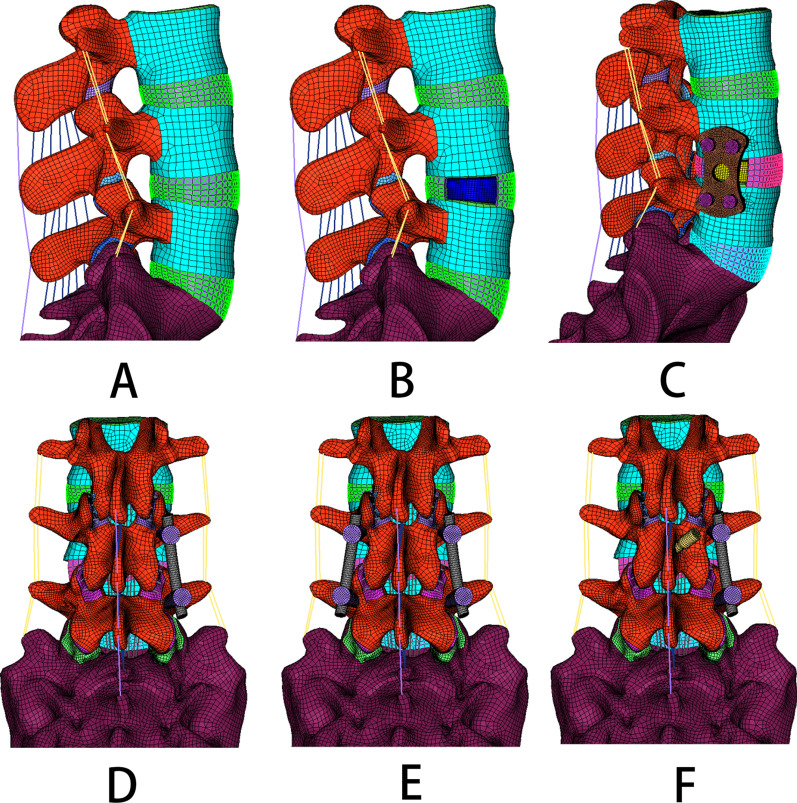
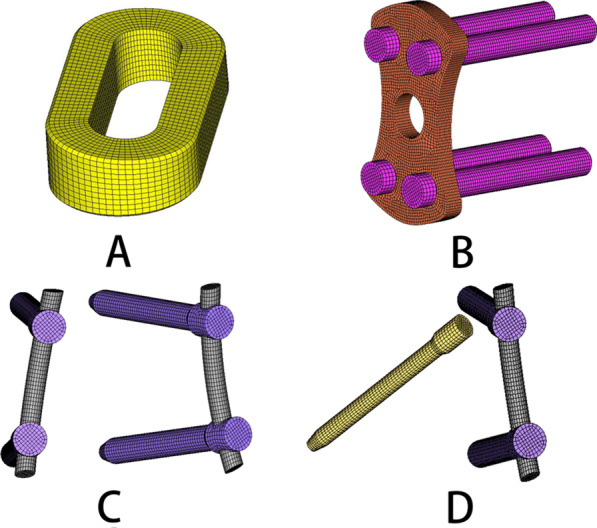
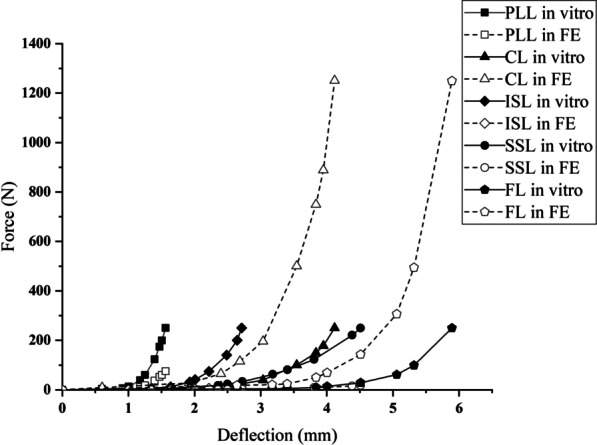
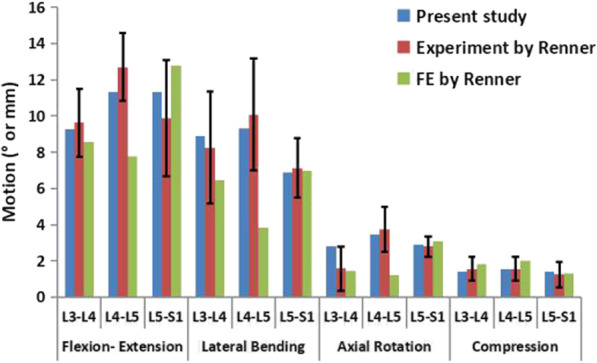
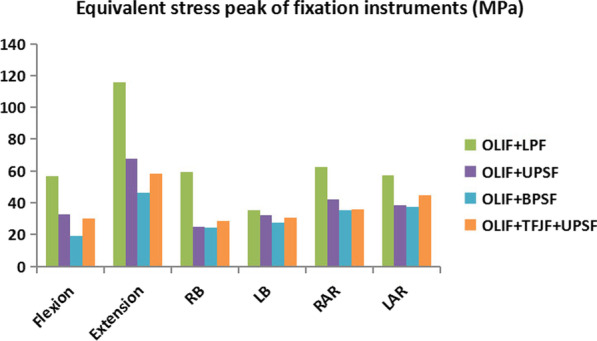
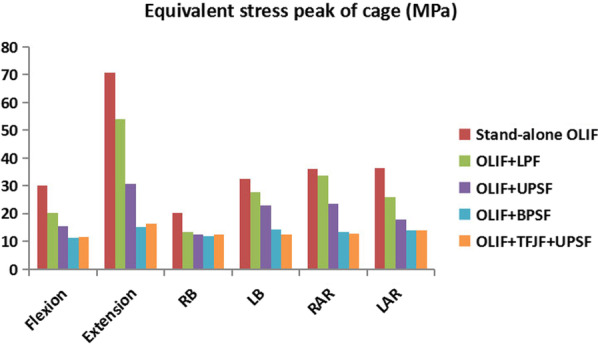
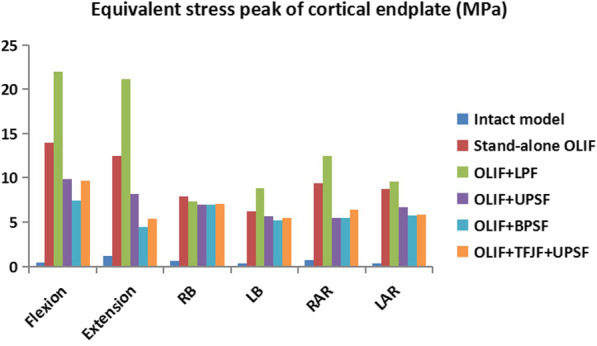
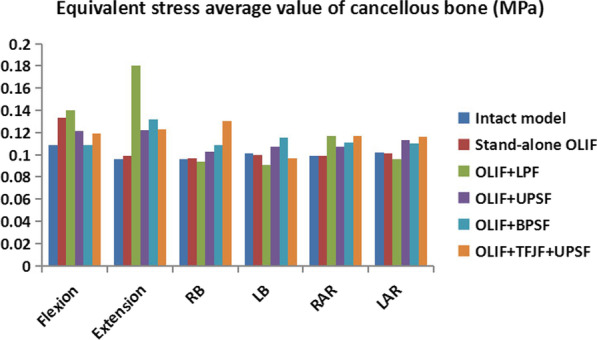
Methods: A three-dimensional nonlinear finite element (FE) model of an intact L3-S1 lumbar spine was built and validated. The intact model was modified to develop five OLIF surgery models (Stand-alone OLIF; OLIF with lateral plate fixation [OLIF + LPF]; OLIF with unilateral pedicle screws fixation [OLIF + UPSF]; OLIF with bilateral pedicle screws fixation [OLIF + BPSF]; OLIF with translaminar facet joint fixation + unilateral pedicle screws fixation [OLIF + TFJF + UPSF]) in which the surgical segment was L4-L5. Under a follower load of 500 N, a 7.5-Nm moment was applied to all lumbar spine models to calculate the range of motion (ROM), equivalent stress peak of fixation instruments (ESPFI), equivalent stress peak of cage (ESPC), equivalent stress peak of cortical endplate (ESPCE), and equivalent stress average value of cancellous bone (ESAVCB).
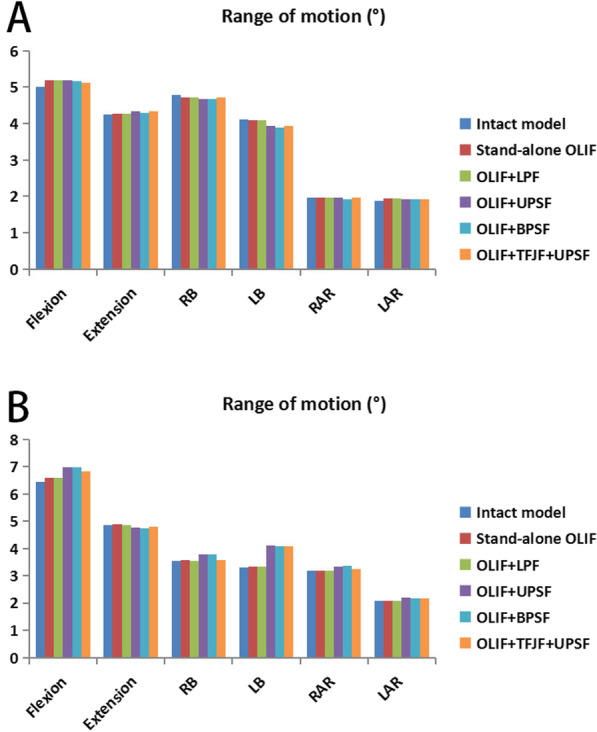
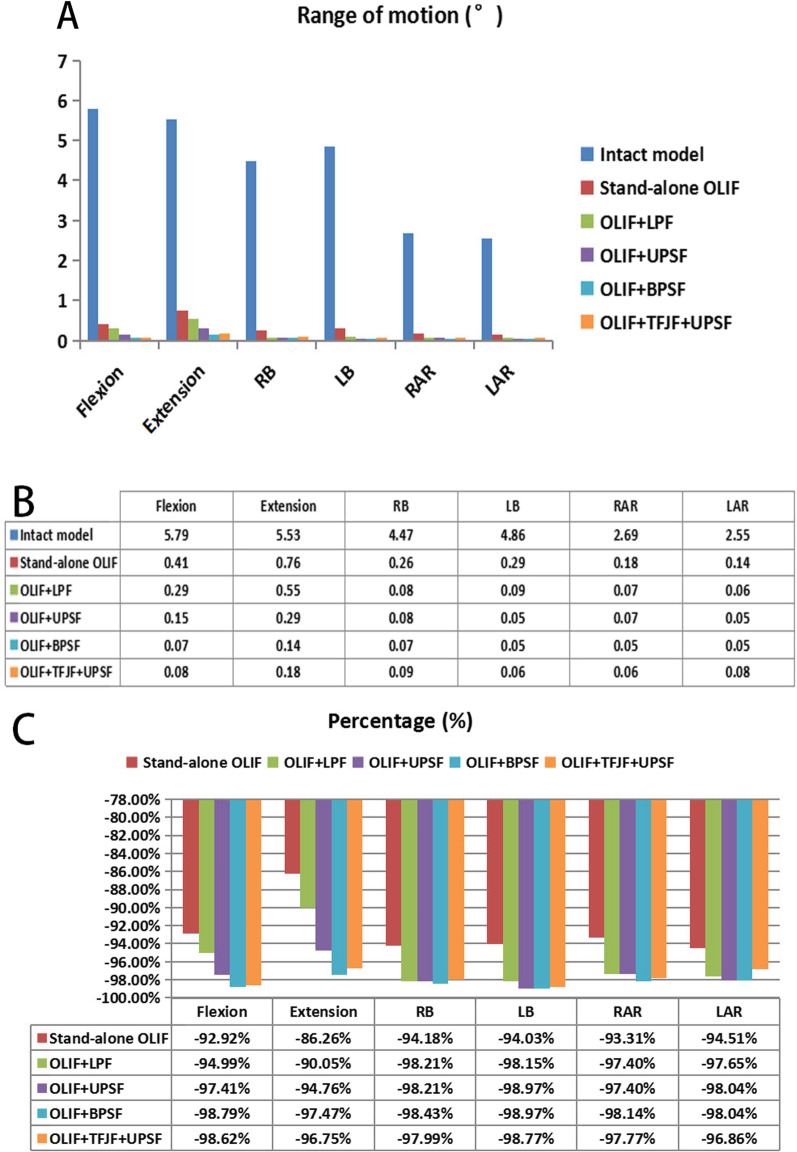
Results: Compared with the intact model, the ROM of the L4-L5 segment in each OLIF surgery model decreased by > 80%. The ROM values of adjacent segments were not significantly different. The ESPFI, ESPC, and ESPCE values of the OLIF + BPSF model were smaller than those of the other OLIF surgery models. The ESAVCB value of the normal lumbar model was less than the ESAVCB values of all OLIF surgical models. In most postures, the ESPFI, ESPCE, and ESAVCB values of the OLIF + LPF model were the largest. The ESPC was higher in the Stand-alone OLIF model than in the other OLIF models. The stresses of several important components of the OLIF + UPSF and OLIF + TFJF + UPSF models were between those of the OLIF + LPF and OLIF + BPSF models.
Conclusions: Our biomechanical FE analysis indicated the greater ability of OLIF + BPSF to retain lumbar stability, resist cage subsidence, and maintain disc height. Therefore, in the augmentation of OLIF, bilateral pedicle screws fixation may be the best approach.
Keywords: Augmentation; Biomechanical study; Finite element analysis; Lumbar spine; Oblique lumbar interbody fusion.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Biomechanical differences between two different shapes of oblique lumbar interbody fusion cages on whether to add posterior internal fixation system: a finite element analysis.J Orthop Surg Res. 2023 Dec 13;18(1):962. doi: 10.1186/s13018-023-04461-6. J Orthop Surg Res. 2023. PMID: 38093357 Free PMC article.
-
Biomechanical Comparison of a Novel Facet Joint Fusion Fixation Device With Conventional Pedicle Screw Fixation Device: A Finite Element Analysis.Orthop Surg. 2025 Apr;17(4):1230-1242. doi: 10.1111/os.70003. Epub 2025 Feb 27. Orthop Surg. 2025. PMID: 40016885 Free PMC article.
-
Effects of osteoporosis on the biomechanics of various supplemental fixations co-applied with oblique lumbar interbody fusion (OLIF): a finite element analysis.BMC Musculoskelet Disord. 2022 Aug 19;23(1):794. doi: 10.1186/s12891-022-05645-7. BMC Musculoskelet Disord. 2022. PMID: 35986271 Free PMC article.
-
Biomechanical Comparison of Stand-Alone and Bilateral Pedicle Screw Fixation for Oblique Lumbar Interbody Fusion Surgery-A Finite Element Analysis.World Neurosurg. 2020 Sep;141:e204-e212. doi: 10.1016/j.wneu.2020.05.245. Epub 2020 Jun 2. World Neurosurg. 2020. PMID: 32502627
-
Influence of double rods and interbody cages on range of motion and rod stress after spinopelvic instrumentation: a finite element study.Eur Spine J. 2022 Jun;31(6):1515-1524. doi: 10.1007/s00586-022-07149-3. Epub 2022 Apr 23. Eur Spine J. 2022. PMID: 35461384 Review.
Cited by
-
Biomechanical Analysis of Double-Level Oblique Lumbar Fusion with Different Types of Fixation: A Finite Element-Based Study.Orthop Surg. 2023 May;15(5):1357-1365. doi: 10.1111/os.13703. Epub 2023 Apr 18. Orthop Surg. 2023. PMID: 37073100 Free PMC article.
-
Finite element analysis of biomechanical investigation on diverse internal fixation techniques in oblique lumbar interbody fusion.BMC Musculoskelet Disord. 2024 Oct 12;25(1):804. doi: 10.1186/s12891-024-07887-z. BMC Musculoskelet Disord. 2024. PMID: 39395967 Free PMC article.
-
Biomechanical differences between two different shapes of oblique lumbar interbody fusion cages on whether to add posterior internal fixation system: a finite element analysis.J Orthop Surg Res. 2023 Dec 13;18(1):962. doi: 10.1186/s13018-023-04461-6. J Orthop Surg Res. 2023. PMID: 38093357 Free PMC article.
-
Novel Instruments for Full Endoscopic Trans-Kambin Triangle Lumbar Interbody Fusion With Reverse Oblique Lateral Cage Insertion: A Case Report and Technical Note.Int J Spine Surg. 2025 Mar 6;19(1):63-69. doi: 10.14444/8695. Int J Spine Surg. 2025. PMID: 40049732 Free PMC article.
-
Biomechanical characteristics of 2 different posterior fixation methods of bilateral pedicle screws: A finite element analysis.Medicine (Baltimore). 2022 Sep 9;101(36):e30419. doi: 10.1097/MD.0000000000030419. Medicine (Baltimore). 2022. PMID: 36086784 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
