

Proximal junctional fractures after long-segment instrumented fusion: comparisons between upper instrumented vertebrae and upper instrumented vertebrae + 1
- PMID: 35568929
- PMCID: PMC9107646
- DOI: 10.1186/s13018-022-03173-7
Proximal junctional fractures after long-segment instrumented fusion: comparisons between upper instrumented vertebrae and upper instrumented vertebrae + 1
Abstract
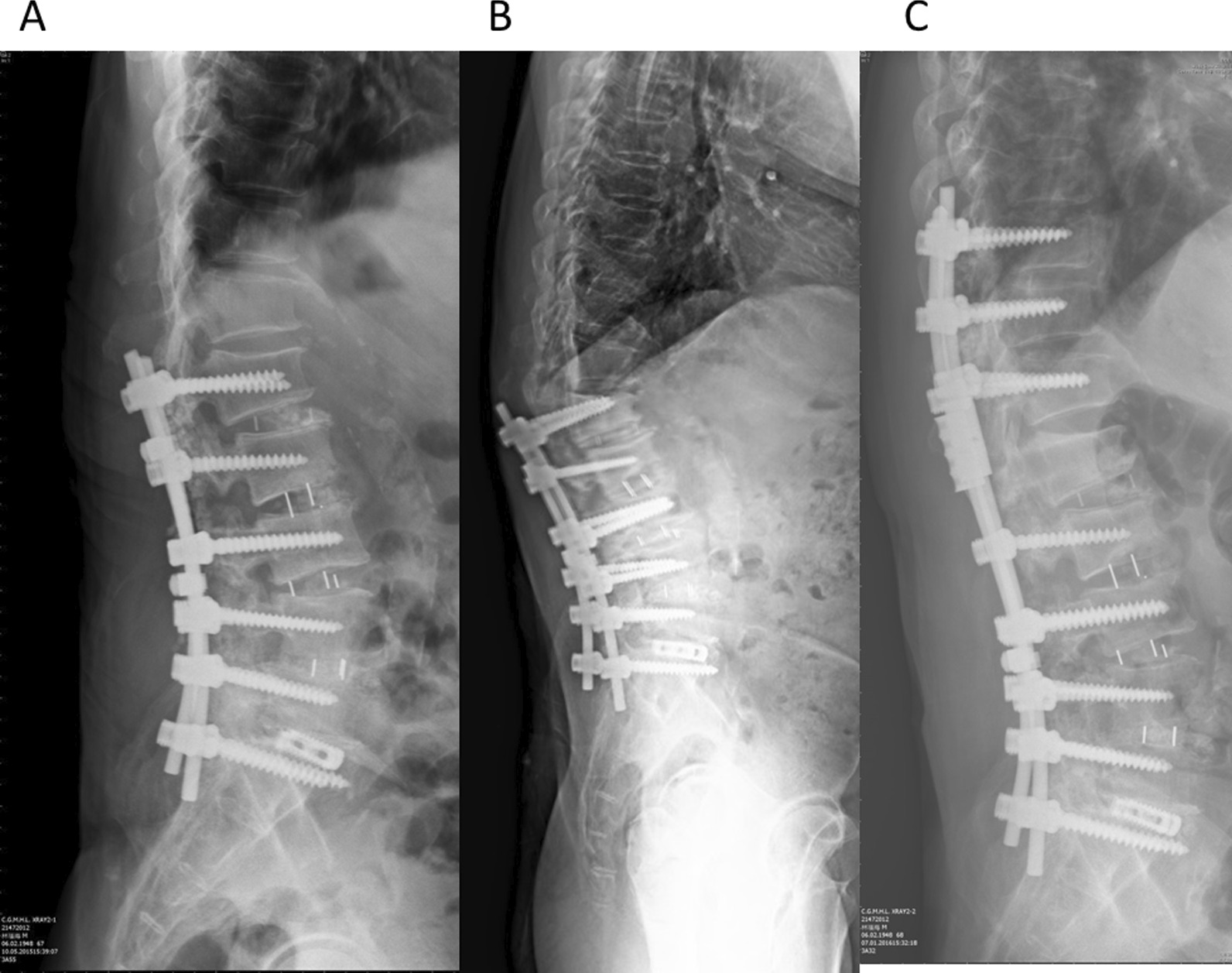
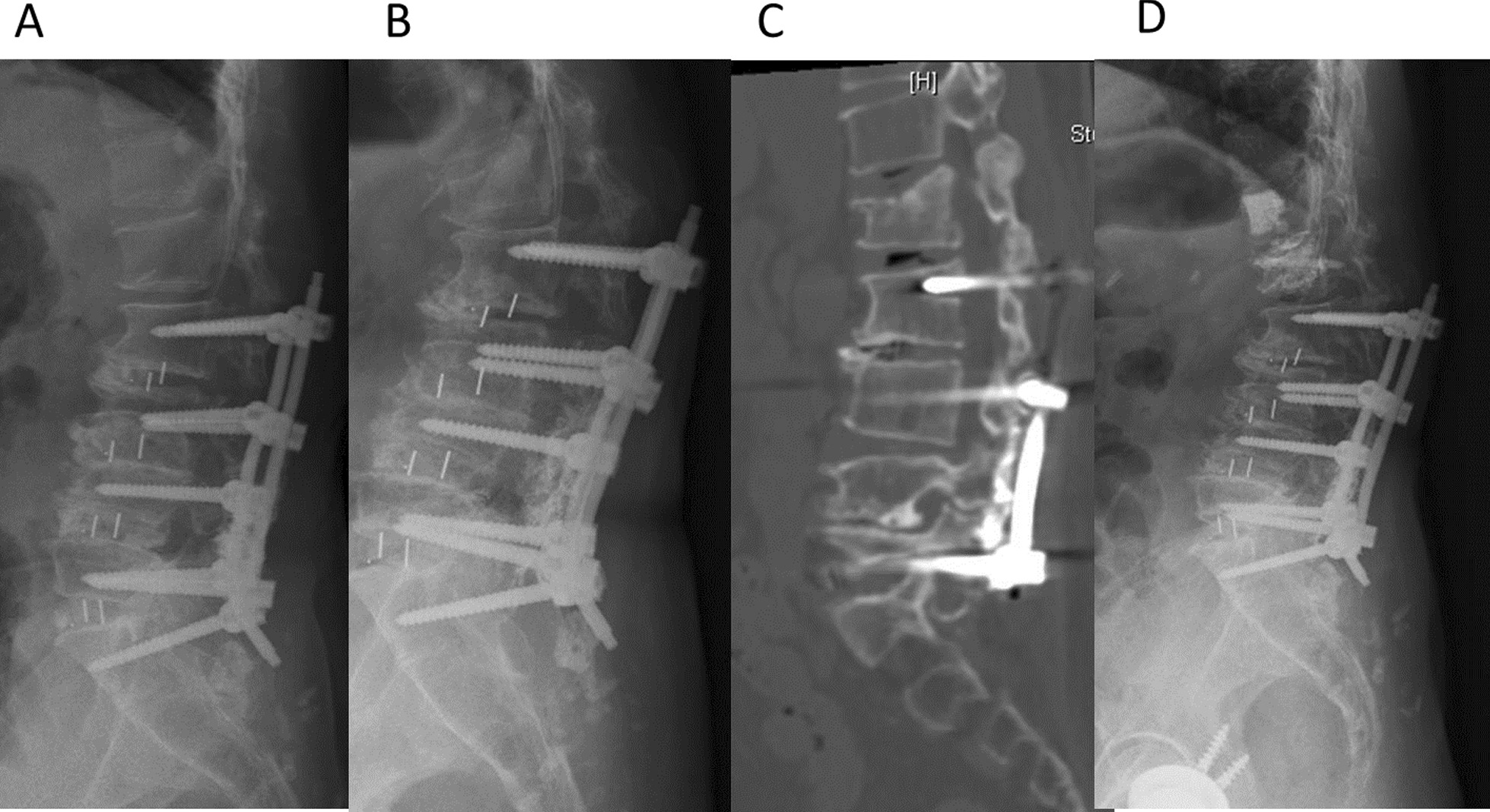
Introduction: Proximal junctional failure (PJF) is a well-known complication after long-segment (at least 4 vertebral levels) instrumented fusion. The etiologies of PJF include degenerative processes or are fracture induced. The fracture type of PJF includes vertebral fractures developed at the upper instrumented vertebrae (UIV) or UIV + 1. The purpose of this study was to investigate clinical and radiographic features of these two subtypes of PJF and to analyze risk factors in these patients.
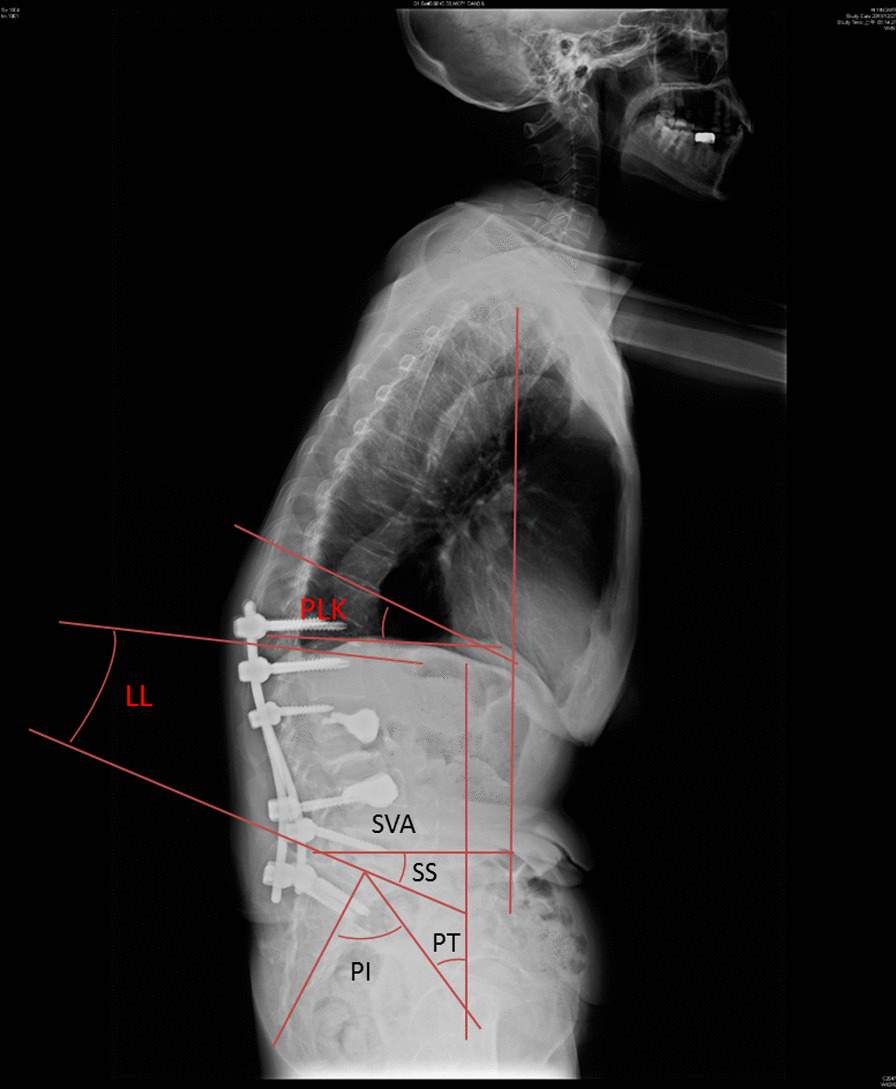
Method: In total, forty-two patients with PJF who underwent revision surgery were included. Twenty patients suffered fractures at the UIV, and the other 22 cases had fractures at UIV + 1. The weighted Charlson Comorbidity Index (CCI) and bone mineral density (BMD) T scores for these patients were recorded. Surgery-related data of index surgery and complications were collected. Radiographic parameters including pelvic tilt (PT), pelvic incidence (PI), sagittal vertical axis (SVA), lumbar lordosis (LL), and PI-LL were recorded in both groups before and after the revision surgery.
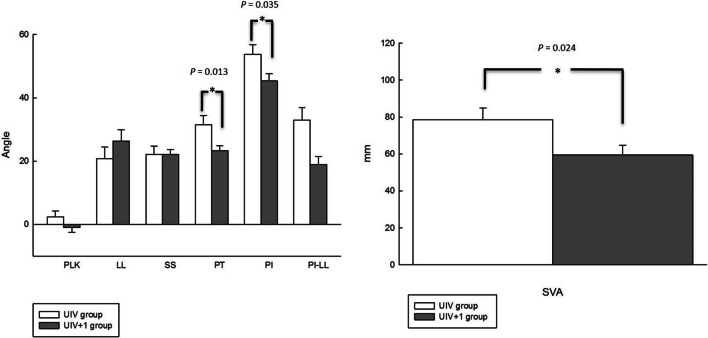
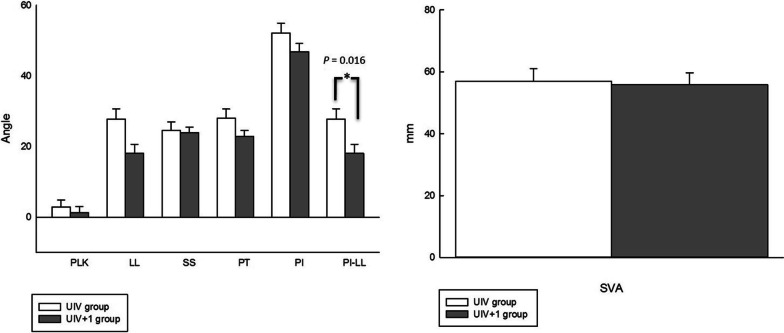
Result: Both groups had severe osteoporosis and comorbidities. The interval between the index surgery and revision surgery was shorter in the UIV group than in the UIV + 1 group (8.2 months vs. 35.9 months; p < 0.001). The analysis for radiographic parameters in UIV and UIV + 1 group demonstrated no significant change before and after the revision surgery. However, the preoperative radiographic analysis showed a larger PT (31.5° vs. 23.2°, p = 0.013), PI (53.7° vs. 45.3°, p = 0.035), and SVA (78.6° vs. 59.4°, p = 0.024) in the UIV group compared to the UIV + 1 group. The postoperative radiographic analysis showed a larger PI-LL (27.8° vs. 18.1°, p = 0.016) in the UIV group compared to the UIV + 1 group.
Conclusion: PJF in the UIV group tends to occur earlier than in the UIV + 1 group. Moreover, more severe global sagittal imbalances were found in the UIV group than in UIV + 1 group.
© 2022. The Author(s).
Conflict of interest statement
The author declares that there no conflicts of interest regarding the publication of this paper.
Figures
References
-
- Theologis AA, Miller L, Callahan M, Lau D, Zygourakis C, Scheer JK, Burch S, Pekmezci M, Chou D, Tay B, Mummaneni P, Berven S, Deviren V, Ames CP. Economic impact of revision surgery for proximal junctional failure after adult spinal deformity surgery: a cost analysis of 57 operations in a 10-year experience at a major deformity center. Spine. 2016;41:E964–E972. doi: 10.1097/BRS.0000000000001523. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
