

A standardized implementation of multicenter quality improvement program of very low birth weight newborns could significantly reduce admission hypothermia and improve outcomes
- PMID: 35568937
- PMCID: PMC9107002
- DOI: 10.1186/s12887-022-03310-5
A standardized implementation of multicenter quality improvement program of very low birth weight newborns could significantly reduce admission hypothermia and improve outcomes
Abstract
Background: Admission hypothermia (AH, < 36.5℃) remains a major challenge for global neonatal survival, especially in developing countries. Baseline research shows nearly 89.3% of very low birth weight (VLBW, < 1500 g) infants suffer from AH in China. Therefore, a prospective multicentric quality improvement (QI) initiative to reduce regional AH and improve outcomes among VLBW neonates was implemented.
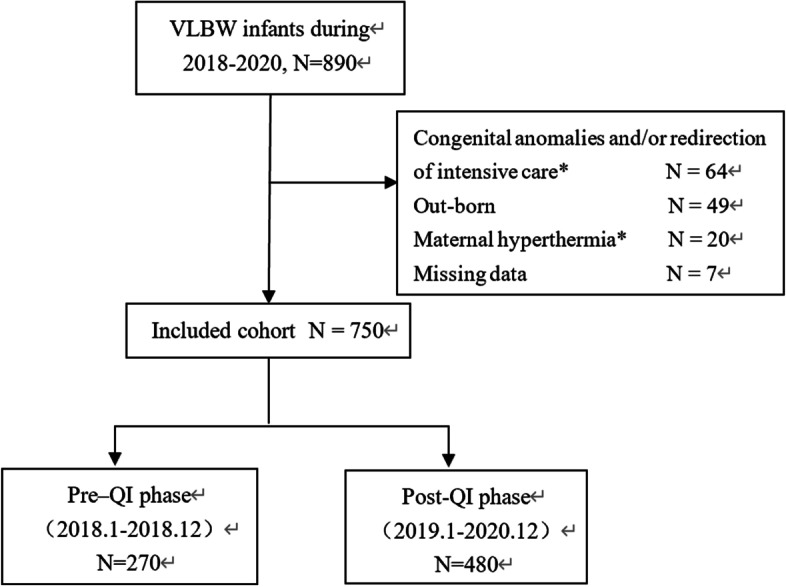
Methods: The study used a sequential Plan-Do-Study-Act (PDSA) approach. Clinical data were collected prospectively from 5 NICUs within the Sino-Northern Neonatal Network (SNN) in China. The hypothermia prevention bundle came into practice on January 1, 2019. The clinical characteristics and outcomes data in the pre-QI phase (January 1, 2018- December 31, 2018) were compared with that from the post-QI phase (January 1, 2019-December 31, 2020). Clinical characteristics and outcomes data were analyzed.
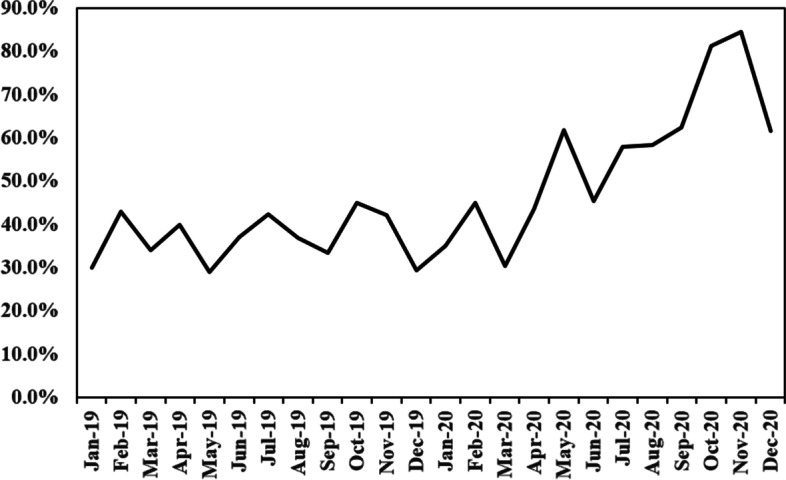
Results: A total of 750 in-born VLBW infants were enrolled in the study, 270 in the pre-QI period and 480 in the post- QI period, respectively. There were no significant differences in clinical characteristics of infants between these two phases. Compared with pre-QI period, the incidence of AH was decreased significantly after the QI initiative implementation in the post-QI period (95.9% vs. 71.3%, P < 0.01). Incidence of admission moderate-to-severe hypothermia (AMSH, < 36℃) also decreased significantly, manifesting a reduction to 38.5% in the post-QI (68.5% vs 30%, P < 0.01). Average admission temperature improved from after QI (35.5 [Formula: see text] 0.7℃ vs. 36.0 [Formula: see text] 0.6℃, P < 0.01). There was no increase in proportion the number of infants with a temperature of > 37.5 °C or thermal burns between the two groups. The risk ratio of mortality in infants during the post-QI period was significantly lower in the post-QI period as compared to the pre-QI period [adjusted risk ratio (aRR): 0.26, 95% confidence interval (CI): 0.13-0.50]. The risk ratio of late-onset neonatal sepsis (LOS) also significantly lowered in the post-QI period (aRR: 0.66, 95% CI: 0.50-0.87).
Conclusion: Implementation of multicentric thermoregulatory QI resulted in a significant reduction in AH and AMSH in VLBW neonates with associated reduction in mortality. We gained a lot from the QI, and successfully aroused the attention of perinatal medical staff to neonatal AH. This provided a premise for continuous quality improvement of AH in the future, and might provide a reference for implementation of similar interventions in developing countries.
Trial registration: Trial registration number: ChiCTR1900020861 . Date of registration: 21 January 2019(21/01/2019). Prospectively registered.
Keywords: Hypothermia; Neonates; Outcomes; Quality improvement; Very low birth weight.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
No financial or nonfinancial benefits have been received or will be received from any party related directly or indirectly to the subject of this article.
Figures

Similar articles
-
Quality improvement bundles to decrease hypothermia in very low/extremely low birth weight infants at birth: a systematic review and meta-analysis.PeerJ. 2024 Nov 1;12:e18425. doi: 10.7717/peerj.18425. eCollection 2024. PeerJ. 2024. PMID: 39498294 Free PMC article.
-
Implementation of a temperature bundle improves admission hypothermia in very-low-birth-weight infants in China: a multicentre study.BMJ Open Qual. 2022 May;11(2):e001407. doi: 10.1136/bmjoq-2021-001407. BMJ Open Qual. 2022. PMID: 35500935 Free PMC article.
-
The impact of a quality improvement project to reduce admission hypothermia on mortality and morbidity in very low birth weight infants.Eur J Pediatr. 2020 Dec;179(12):1851-1858. doi: 10.1007/s00431-020-03711-7. Epub 2020 Jun 6. Eur J Pediatr. 2020. PMID: 32506219
-
Association between admission hypothermia and outcomes in very low birth weight infants in China: a multicentre prospective study.BMC Pediatr. 2020 Jun 29;20(1):321. doi: 10.1186/s12887-020-02221-7. BMC Pediatr. 2020. PMID: 32600275 Free PMC article.
-
The effect of thermoregulation quality improvement initiatives on the admission temperature of premature/very low birth-weight infants in neonatal intensive care units: A systematic review.J Spec Pediatr Nurs. 2020 Apr;25(2):e12286. doi: 10.1111/jspn.12286. Epub 2020 Jan 7. J Spec Pediatr Nurs. 2020. PMID: 31909894
Cited by
-
Association between Neonatal Outcomes and Admission Hypothermia among Very Preterm Infants in Chinese Neonatal Intensive Care Units: A Multicenter Cohort Study.Am J Perinatol. 2024 Dec;41(16):2298-2307. doi: 10.1055/s-0044-1786873. Epub 2024 May 27. Am J Perinatol. 2024. PMID: 38802079 Free PMC article.
-
The Chinese adverse prognosis of very preterm infants (CARE-Preterm) cohort: study design and baseline characteristics for a prospective multicenter cohort study.BMC Pediatr. 2025 May 13;25(1):377. doi: 10.1186/s12887-025-05722-5. BMC Pediatr. 2025. PMID: 40361046 Free PMC article.
-
Quality improvement bundles to decrease hypothermia in very low/extremely low birth weight infants at birth: a systematic review and meta-analysis.PeerJ. 2024 Nov 1;12:e18425. doi: 10.7717/peerj.18425. eCollection 2024. PeerJ. 2024. PMID: 39498294 Free PMC article.
-
Development and validation of a model to predict mortality risk among extremely preterm infants during the early postnatal period: a multicentre prospective cohort study.BMJ Open. 2023 Dec 28;13(12):e074309. doi: 10.1136/bmjopen-2023-074309. BMJ Open. 2023. PMID: 38154879 Free PMC article.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
