

Infarct size, inflammatory burden, and admission hyperglycemia in diabetic patients with acute myocardial infarction treated with SGLT2-inhibitors: a multicenter international registry
- PMID: 35570280
- PMCID: PMC9107763
- DOI: 10.1186/s12933-022-01506-8
Infarct size, inflammatory burden, and admission hyperglycemia in diabetic patients with acute myocardial infarction treated with SGLT2-inhibitors: a multicenter international registry
Abstract
Background: The inflammatory response occurring in acute myocardial infarction (AMI) has been proposed as a potential pharmacological target. Sodium-glucose co-transporter 2 inhibitors (SGLT2-I) currently receive intense clinical interest in patients with and without diabetes mellitus (DM) for their pleiotropic beneficial effects. We tested the hypothesis that SGLT2-I have anti-inflammatory effects along with glucose-lowering properties. Therefore, we investigated the link between stress hyperglycemia, inflammatory burden, and infarct size in a cohort of type 2 diabetic patients presenting with AMI treated with SGLT2-I versus other oral anti-diabetic (OAD) agents.
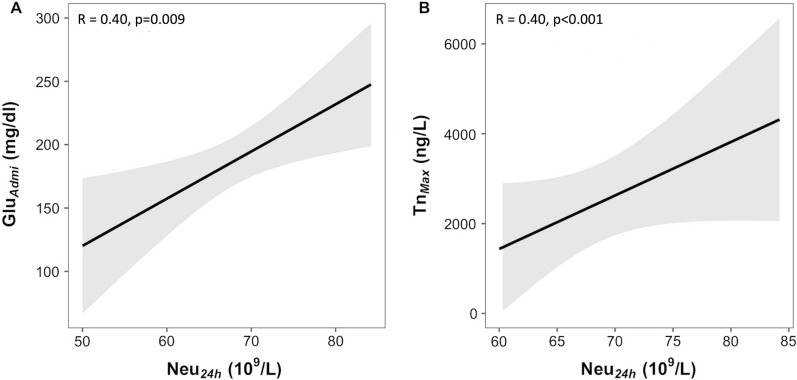
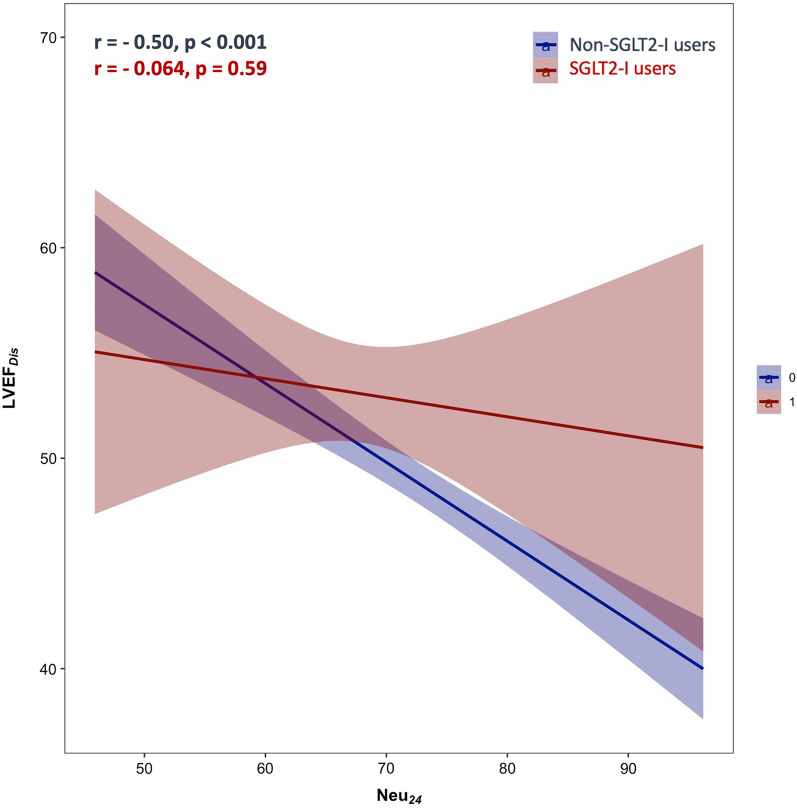
Methods: In this multicenter international observational registry, consecutive diabetic AMI patients undergoing percutaneous coronary intervention (PCI) between 2018 and 2021 were enrolled. Based on the presence of anti-diabetic therapy at the admission, patients were divided into those receiving SGLT2-I (SGLT-I users) versus other OAD agents (non-SGLT2-I users). The following inflammatory markers were evaluated at different time points: white-blood-cell count, neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), neutrophil-to-platelet ratio (NPR), and C-reactive protein. Infarct size was assessed by echocardiography and by peak troponin levels.
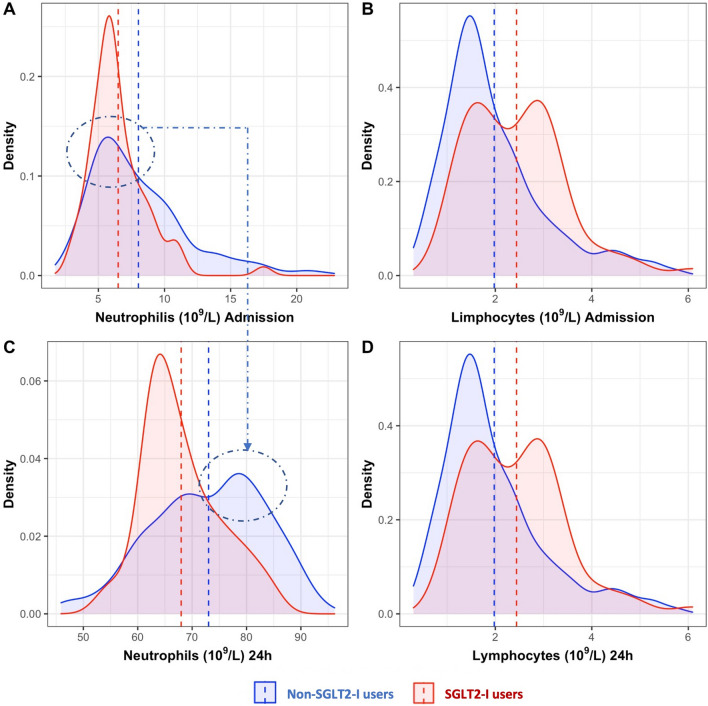
Results: The study population consisted of 583 AMI patients (with or without ST-segment elevation): 98 SGLT2-I users and 485 non-SGLT-I users. Hyperglycemia at admission was less prevalent in the SGLT2-I group. Smaller infarct size was observed in patients treated with SGLT2-I compared to non-SGLT2-I group. On admission and at 24 h, inflammatory indices were significantly higher in non-SGLT2-I users compared to SGLT2-I patients, with a significant increase in neutrophil levels at 24 h. At multivariable analysis, the use of SGLT2-I was a significant predictor of reduced inflammatory response (OR 0.457, 95% CI 0.275-0.758, p = 0.002), independently of age, admission creatinine values, and admission glycemia. Conversely, peak troponin values and NSTEMI occurrence were independent predictors of a higher inflammatory status.
Conclusions: Type 2 diabetic AMI patients receiving SGLT2-I exhibited significantly reduced inflammatory response and smaller infarct size compared to those receiving other OAD agents, independently of glucose-metabolic control. Our findings are hypothesis generating and provide new insights on the cardioprotective effects of SGLT2-I in the setting of coronary artery disease.
Trial registration: Data are part of the ongoing observational registry: SGLT2-I AMI PROTECT.
Clinicaltrials: gov Identifier: NCT05261867.
Keywords: Acute myocardial infarction; Hyperglycemia; Infarct size; Inflammation; SGLT2-I.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
