

Arterial vasodilation drives convective fluid flow in the brain: a poroelastic model
- PMID: 35570287
- PMCID: PMC9107702
- DOI: 10.1186/s12987-022-00326-y
Arterial vasodilation drives convective fluid flow in the brain: a poroelastic model
Abstract
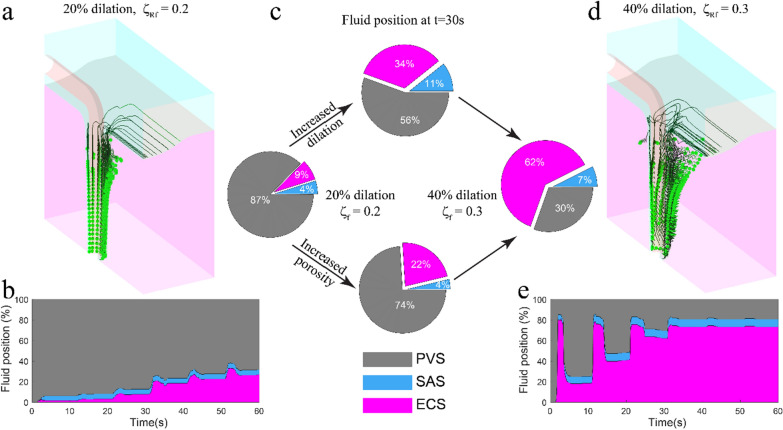
The movement of fluid into, through, and out of the brain plays an important role in clearing metabolic waste. However, there is controversy regarding the mechanisms driving fluid movement in the fluid-filled paravascular spaces (PVS), and whether the movement of metabolic waste in the brain extracellular space (ECS) is primarily driven by diffusion or convection. The dilation of penetrating arterioles in the brain in response to increases in neural activity (neurovascular coupling) is an attractive candidate for driving fluid circulation, as it drives deformation of the brain tissue and of the PVS around arteries, resulting in fluid movement. We simulated the effects of vasodilation on fluid movement into and out of the brain ECS using a novel poroelastic model of brain tissue. We found that arteriolar dilations could drive convective flow through the ECS radially outward from the arteriole, and that this flow is sensitive to the dynamics of the dilation. Simulations of sleep-like conditions, with larger vasodilations and increased extracellular volume in the brain showed enhanced movement of fluid from the PVS into the ECS. Our simulations suggest that both sensory-evoked and sleep-related arteriolar dilations can drive convective flow of cerebrospinal fluid not just in the PVS, but also into the ECS through the PVS around arterioles.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




Similar articles
-
Functional hyperemia drives fluid exchange in the paravascular space.Fluids Barriers CNS. 2020 Aug 20;17(1):52. doi: 10.1186/s12987-020-00214-3. Fluids Barriers CNS. 2020. PMID: 32819402 Free PMC article.
-
The role of brain barriers in fluid movement in the CNS: is there a 'glymphatic' system?Acta Neuropathol. 2018 Mar;135(3):387-407. doi: 10.1007/s00401-018-1812-4. Epub 2018 Feb 10. Acta Neuropathol. 2018. PMID: 29428972 Review.
-
Spatial model of convective solute transport in brain extracellular space does not support a "glymphatic" mechanism.J Gen Physiol. 2016 Dec;148(6):489-501. doi: 10.1085/jgp.201611684. Epub 2016 Nov 11. J Gen Physiol. 2016. PMID: 27836940 Free PMC article.
-
Evidence for a 'paravascular' fluid circulation in the mammalian central nervous system, provided by the rapid distribution of tracer protein throughout the brain from the subarachnoid space.Brain Res. 1985 Feb 4;326(1):47-63. doi: 10.1016/0006-8993(85)91383-6. Brain Res. 1985. PMID: 3971148
-
Local diffusion in the extracellular space of the brain.Neurobiol Dis. 2023 Feb;177:105981. doi: 10.1016/j.nbd.2022.105981. Epub 2022 Dec 26. Neurobiol Dis. 2023. PMID: 36581229 Review.
Cited by
-
Low-intensity pulsed ultrasound stimulation (LIPUS) modulates microglial activation following intracortical microelectrode implantation.Nat Commun. 2024 Jun 29;15(1):5512. doi: 10.1038/s41467-024-49709-9. Nat Commun. 2024. PMID: 38951525 Free PMC article.
-
Long-wavelength traveling waves of vasomotion modulate the perfusion of cortex.Neuron. 2024 Jul 17;112(14):2349-2367.e8. doi: 10.1016/j.neuron.2024.04.034. Epub 2024 May 22. Neuron. 2024. PMID: 38781972 Free PMC article.
-
Neural activity induces strongly coupled electro-chemo-mechanical interactions and fluid flow in astrocyte networks and extracellular space-A computational study.PLoS Comput Biol. 2023 Jul 21;19(7):e1010996. doi: 10.1371/journal.pcbi.1010996. eCollection 2023 Jul. PLoS Comput Biol. 2023. PMID: 37478153 Free PMC article.
-
Perivascular interactions and tissue properties modulate directional glymphatic transport in the brain.Fluids Barriers CNS. 2025 Jun 23;22(1):63. doi: 10.1186/s12987-025-00668-3. Fluids Barriers CNS. 2025. PMID: 40551200 Free PMC article.
-
The glymphatic system: Current understanding and modeling.iScience. 2022 Aug 20;25(9):104987. doi: 10.1016/j.isci.2022.104987. eCollection 2022 Sep 16. iScience. 2022. PMID: 36093063 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
