Deconstructive repair of a traumatic vertebrovertebral arteriovenous fistula via a contralateral endovascular approach
- PMID: 35570470
- PMCID: PMC9537651
- DOI: 10.7461/jcen.2022.E2021.10.002
Deconstructive repair of a traumatic vertebrovertebral arteriovenous fistula via a contralateral endovascular approach
Abstract
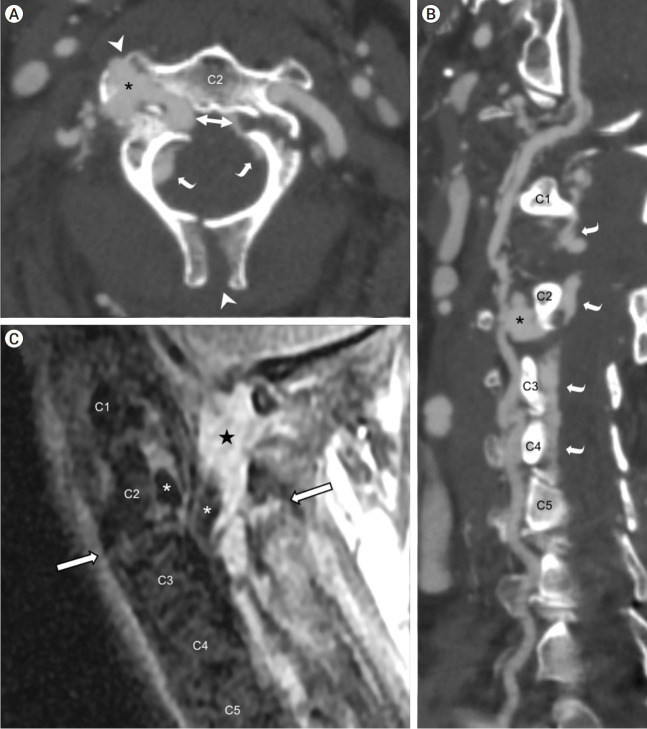
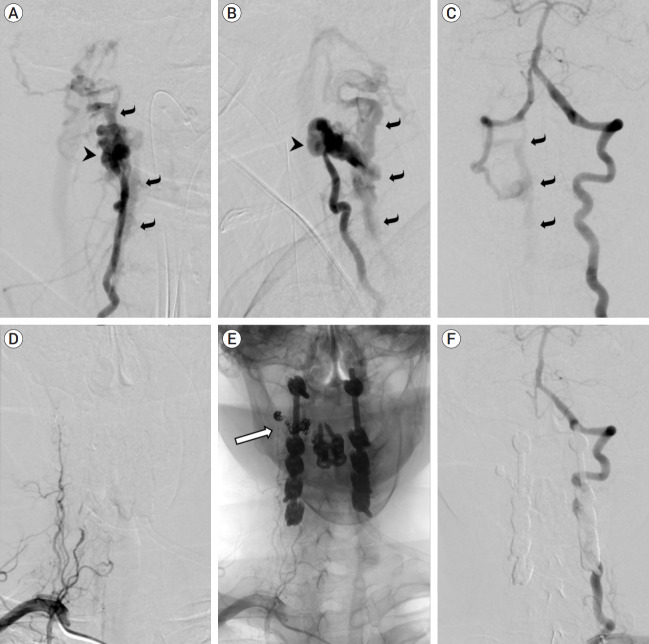
Vertebrovertebral arteriovenous fistulas (VVAVFs) are rare entities that lack consensus guidelines for their management. Our case describes the successful treatment of a traumatic VVAVF via a contralateral deconstructive endovascular approach. A 64-year-old female presented following a traumatic fall. Computed tomography angiogram highlighted a 2 cm pseudoaneurysm of the right vertebral artery (VA) with epidural contrast enhancement and a hematoma with flow voids within the epidural space. Digital subtraction angiography showed a VVAVF at C2-3 with retrograde filling of the distal right VA. Having undergone several unsuccessful passes of the proximal dissection flap in the right VA, the patient underwent a contralateral deconstructive approach with correction of the VVAVF without complication. The remaining feeding branches had occluded after 1 week. The patient made a complete recovery without neurological sequelae at 3-month follow-up.
Keywords: Arteriovenous fistula; Endovascular; Endovascular procedures; Fistula; Vertebral artery.
Figures
Similar articles
-
Endovascular stent-graft treatment for a traumatic vertebrovertebral arteriovenous fistula with pseudoaneurysm.Ann Vasc Surg. 2014 Feb;28(2):489.e11-4. doi: 10.1016/j.avsg.2012.12.013. Epub 2013 Nov 5. Ann Vasc Surg. 2014. PMID: 24200138
-
Direct Vertebral Artery Puncture During Open Surgery for the Endovascular Treatment of a Recurrent Vertebro-Vertebral Arteriovenous Fistula.World Neurosurg. 2021 Feb;146:166-170. doi: 10.1016/j.wneu.2020.10.156. Epub 2020 Nov 3. World Neurosurg. 2021. PMID: 33152497
-
Endovascular treatment of high-flow cervical direct vertebro-vertebral arteriovenous fistula with detachable coils and Onyx liquid embolic agent.Acta Neurochir (Wien). 2011 Feb;153(2):347-52. doi: 10.1007/s00701-010-0850-z. Epub 2010 Nov 9. Acta Neurochir (Wien). 2011. PMID: 21058042
-
Endovascular management of V3 segment vertebro-vertebral fistula: case management and literature review.Br J Neurosurg. 2024 Oct;38(5):1188-1192. doi: 10.1080/02688697.2022.2071416. Epub 2022 May 3. Br J Neurosurg. 2024. PMID: 35502703 Review.
-
Multi-modal endovascular management of traumatic pseudoaneurysm and arteriovenous fistula of the ascending cervical artery: A technical report and review of literature.Clin Neurol Neurosurg. 2021 Mar;202:106539. doi: 10.1016/j.clineuro.2021.106539. Epub 2021 Feb 2. Clin Neurol Neurosurg. 2021. PMID: 33601270 Review.
Cited by
-
Vertebro-Vertebral Arteriovenous Fistulae: A Case Series of Endovascular Management at a Single Center.Diagnostics (Basel). 2024 Feb 13;14(4):414. doi: 10.3390/diagnostics14040414. Diagnostics (Basel). 2024. PMID: 38396452 Free PMC article.
References
-
- Aljobeh A, Sorenson TJ, Bortolotti C, Cloft H, Lanzino G. Vertebral arteriovenous fistula: a review article. World Neurosurg. 2019 Feb;122:e1388–97. - PubMed
-
- Berenstein A, Lasjaunias P, ter Brugge KG. In: Surgical Neuroangiography. Berenstein A, Lasjaunias P, Brugge KG, editors. New York: Springer-Verlag; 2004. Vertebro-vertebral arteriovenous fistulae; pp. 743–51.
-
- Groen RJ, Groenewegen HJ, van Alphen HA, Hoogland PV. Morphology of the human internal vertebral venous plexus: a cadaver study after intravenous araldite CY 221 injection. Anat Rec. 1997 Oct;249(2):285–94. - PubMed