

Determining the Hierarchy of Coma Recovery Scale-Revised Rating Scale Categories and Alignment with Aspen Consensus Criteria for Patients with Brain Injury: A Rasch Analysis
- PMID: 35570725
- PMCID: PMC9529298
- DOI: 10.1089/neu.2022.0095
Determining the Hierarchy of Coma Recovery Scale-Revised Rating Scale Categories and Alignment with Aspen Consensus Criteria for Patients with Brain Injury: A Rasch Analysis
Abstract
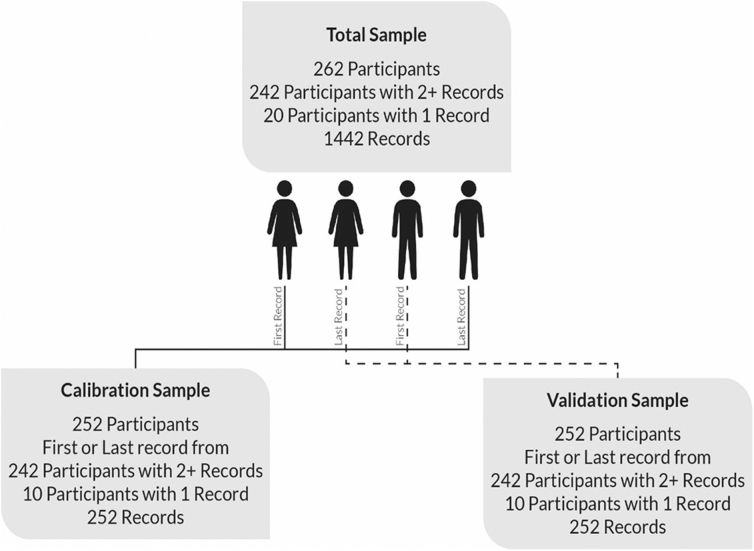
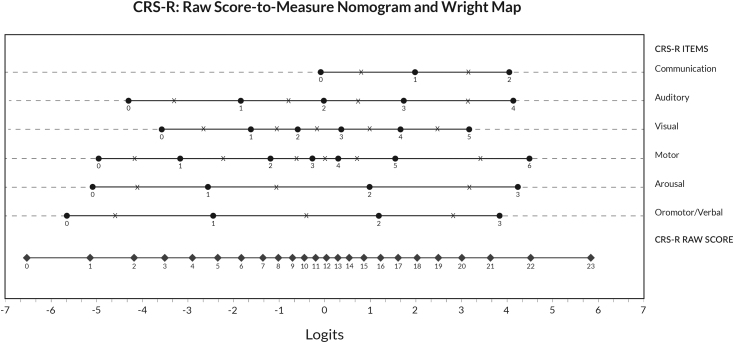
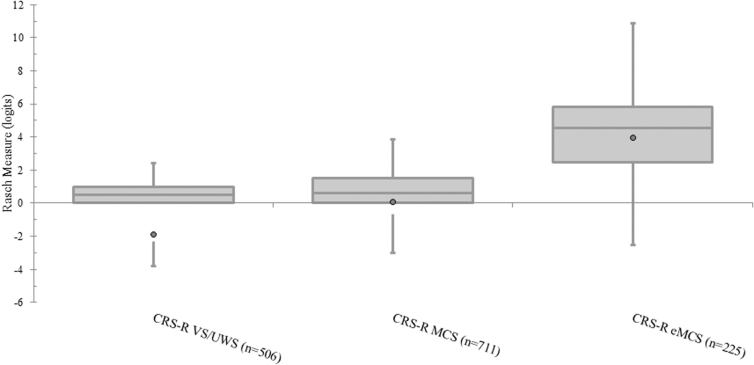
This study aimed to empirically evaluate the hierarchical structure of the Coma Recovery Scale-Revised (CRS-R) rating scale categories and their alignment with the Aspen consensus criteria for determining disorders of consciousness (DoC) following a severe brain injury. CRS-R data from 262 patients with DoC following a severe brain injury were analyzed applying the partial credit Rasch Measurement Model. Rasch Analysis produced logit calibrations for each rating scale category. Twenty-eight of the 29 CRS-R rating scale categories were operationalized to the Aspen consensus criteria. We expected the hierarchical order of the calibrations to reflect Aspen consensus criteria. We also examined the association between the CRS-R Rasch person measures (indicative of performance ability) and states of consciousness as determined by the Aspen consensus criteria. Overall, the order of the 29 rating scale category calibrations reflected current literature regarding the continuum of neurobehavioral function: category 6 "Functional Object Use" of the Motor item was hardest for patients to achieve; category 0 "None" of the Oromotor/Verbal item was easiest to achieve. Of the 29 rating scale categories, six were not ordered as expected. Four rating scale categories reflecting the Vegetative State (VS)/Unresponsive Wakefulness Syndrome (UWS) had higher calibrations (reflecting greater neurobehavioral function) than the easiest Minimally Conscious State (MCS) item (category 2 "Fixation" of the Visual item). Two rating scale categories, one reflecting MCS and one not operationalized to the Aspen consensus criteria, had higher calibrations than the easiest eMCS item (category 2 "Functional: Accurate" of the Communication item). CRS-R person measures (indicating amount of neurobehavioral function) and states of consciousness, based on Aspen consensus criteria, showed a strong correlation (rs = 0.86; p < 0.01). Our study provides empirical evidence for revising the diagnostic criteria for MCS to also include category 2 "Localization to Sound" of the Auditory item and for Emerged from Minimally Conscious State (eMCS) to include category 4 "Consistent Movement to Command" of the Auditory item.
Keywords: brain injury; disorders of consciousness; measurement; outcome assessment.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
The misdiagnosis of prolonged disorders of consciousness by a clinical consensus compared with repeated coma-recovery scale-revised assessment.BMC Neurol. 2020 Sep 12;20(1):343. doi: 10.1186/s12883-020-01924-9. BMC Neurol. 2020. PMID: 32919461 Free PMC article.
-
Neuropsychological assessment through Coma Recovery Scale-Revised and Coma/Near Coma Scale in a sample of pediatric patients with disorder of consciousness.J Neurol. 2023 Feb;270(2):1019-1029. doi: 10.1007/s00415-022-11456-6. Epub 2022 Nov 5. J Neurol. 2023. PMID: 36335241 Free PMC article.
-
Neurobehavioral Progress and Signs of Transition in Children With Prolonged Disorders of Consciousness: A Retrospective Longitudinal Study With the Coma Recovery Scale-Revised.Pediatr Neurol. 2024 Jun;155:187-192. doi: 10.1016/j.pediatrneurol.2024.03.029. Epub 2024 Apr 6. Pediatr Neurol. 2024. PMID: 38677241
-
[Consciousness disorders: vegetative state and minimally conscious state].Przegl Lek. 2013;70(8):595-600. Przegl Lek. 2013. PMID: 24466701 Review. Polish.
-
Definitions, diagnostic criteria, and clinical assessment scales in disorders of consciousness.Handb Clin Neurol. 2025;207:1-13. doi: 10.1016/B978-0-443-13408-1.00011-7. Handb Clin Neurol. 2025. PMID: 39986716 Review.
Cited by
-
Local Neuronal Activity and the Hippocampal Functional Network Can Predict the Recovery of Consciousness in Individuals With Acute Disorders of Consciousness Caused by Neurological Injury.CNS Neurosci Ther. 2024 Nov;30(11):e70108. doi: 10.1111/cns.70108. CNS Neurosci Ther. 2024. PMID: 39508317 Free PMC article.
-
Comparing indices of responsiveness for the Coma Near-Coma Scale with and without pain items: An Exploratory study.Brain Behav. 2023 Aug;13(8):e3120. doi: 10.1002/brb3.3120. Epub 2023 Jun 11. Brain Behav. 2023. PMID: 37303294 Free PMC article.
-
An Early Rehabilitation Favors the Prognosis of Hypertensive Intracerebral Hemorrhage With Acute Disorders of Consciousness: A Retrospective Cohort Study With Propensity Score Matching.Neural Plast. 2025 Apr 24;2025:8144313. doi: 10.1155/np/8144313. eCollection 2025. Neural Plast. 2025. PMID: 40314032 Free PMC article.
-
Interpreting Change in Disorders of Consciousness Using the Coma Recovery Scale-Revised.J Neurotrauma. 2024 Aug;41(15-16):e1996-e2008. doi: 10.1089/neu.2023.0567. Epub 2024 May 10. J Neurotrauma. 2024. PMID: 38613812 Free PMC article.
-
Behavioral assessment scale of consciousness for nonhuman primates: A Delphi study.Sci Prog. 2023 Jul-Sep;106(3):368504231200995. doi: 10.1177/00368504231200995. Sci Prog. 2023. PMID: 37731354 Free PMC article.
References
-
- Giacino JT, Whyte J, Nakase-Richardson R, et al. . Minimum competency recommendations for programs that provide rehabilitation services for persons with disorders of consciousness: a position statement of the American Congress of Rehabilitation Medicine and the National Institute on Disability, Independent Living and Rehabilitation Research Traumatic Brain Injury Model Systems. Arch Phys Med Rehabil 2020;101(6):1072–1089. - PubMed
-
- Giacino JT, Katz DI, Schiff ND, et al. . Practice guideline update recommendations summary: Disorders of consciousness: report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology 2018;91(10):450–460. - PMC - PubMed
-
- Giacino JT, Ashwal S, Childs N, et al. . The minimally conscious state: definition and diagnostic criteria. Neurology 2002;58(3):349–353. - PubMed
-
- Giacino JT. The minimally conscious state: defining the borders of consciousness. Prog Brain Res 2005;150:381–395. - PubMed
-
- Giacino JT, Kalmar K, Whyte J.. The JFK Coma Recovery Scale-Revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil 2004;85(12):2020–2029. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical