

Gastrointestinal Toxicities of Immune Checkpoint Inhibitors Are Associated With Enhanced Tumor Responsiveness and Improved Survival
- PMID: 35572476
- PMCID: PMC9076156
- DOI: 10.14740/gr1491
Gastrointestinal Toxicities of Immune Checkpoint Inhibitors Are Associated With Enhanced Tumor Responsiveness and Improved Survival
Abstract
Background: Immune checkpoint inhibitors (ICIs) are increasingly used to treat advanced malignancies. However, they are associated with the development of multiple gastrointestinal immune-related adverse events (GI-irAEs). We aimed to evaluate the types and severity of GI-irAEs associated with ICI therapy, to identify potential risk factors for developing GI-irAEs and to determine the relationship of GI-irAEs development to tumor responsiveness and overall survival.
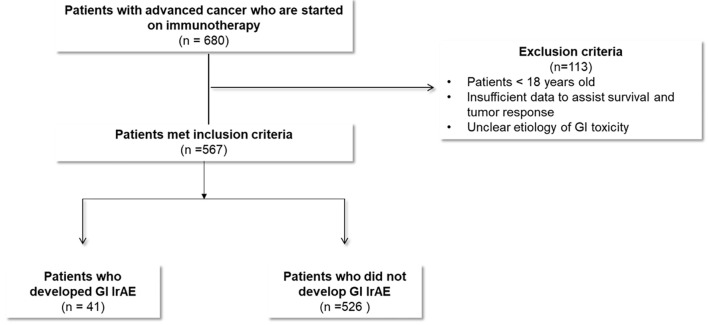
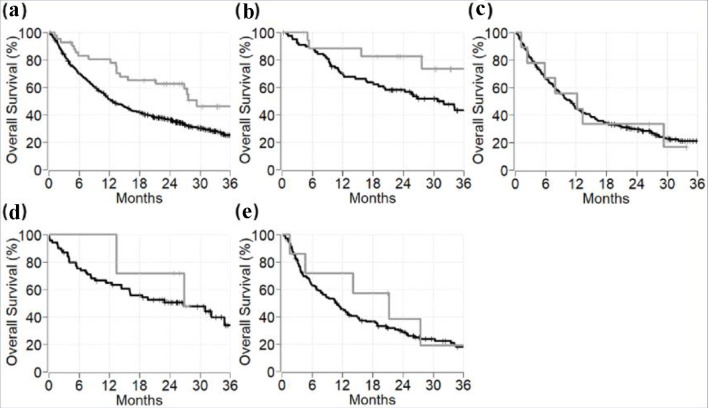
Methods: All patients who received ICIs for advanced malignancies at our center were included. Medical records were reviewed, and data extraction included: baseline demographic characteristics, immunotherapy regimens, development of GI-irAEs, response to treatment, and overall survival. Overall survival was calculated from the date of treatment initiation and estimated by the Kaplan-Meier method.
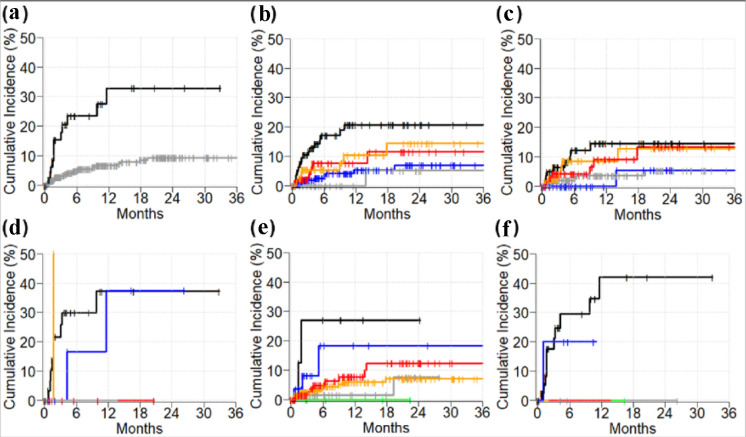
Results: Five hundred sixty-seven patients received ICI therapy for stage IV malignancies. Forty-one (7%) patients experienced at least one GI-irAE. Among those experiencing GI-irAEs, 23 (56%) developed hepatitis, 17 (42%) developed colitis, four (10%) developed pancreatitis, and two (5%) developed gastritis. Patients who developed GI-irAEs experienced a better response to ICI therapy compared to patients who did not develop GI-irAEs (41% vs. 27%, P = 0.003). The 2-year overall survival rate of stage IV cancer patients who developed GI-irAEs was 62% (95% confidence interval (CI): 49 - 79) and 36% for those who did not develop GI-irAEs (95% CI: 32 - 41) (P = 0.002). The median follow-up time of surviving patients was 28 months. Twelve (29%) of the patients receiving dual ICI therapy developed GI-irAEs.
Conclusion: Hepatitis, colitis, and pancreatitis were the most commonly encountered GI-irAEs with ICI therapy. Development of these GI-irAEs was associated with superior tumor responsiveness and better overall survival.
Keywords: Cancer; Gastrointestinal toxicities; Immune checkpoint inhibitors; Immune-related adverse events; Survival; Tumor response.
Copyright 2022, Alomari et al.
Conflict of interest statement
None to declare.
Figures
References
LinkOut - more resources
Full Text Sources