

Hemodynamic deterioration due to increased anterior and posterior cardiac compression during posterior spinal fusion for scoliosis with pectus excavatum
- PMID: 35573103
- PMCID: PMC9096201
- DOI: 10.1177/2050313X221090848
Hemodynamic deterioration due to increased anterior and posterior cardiac compression during posterior spinal fusion for scoliosis with pectus excavatum
Abstract
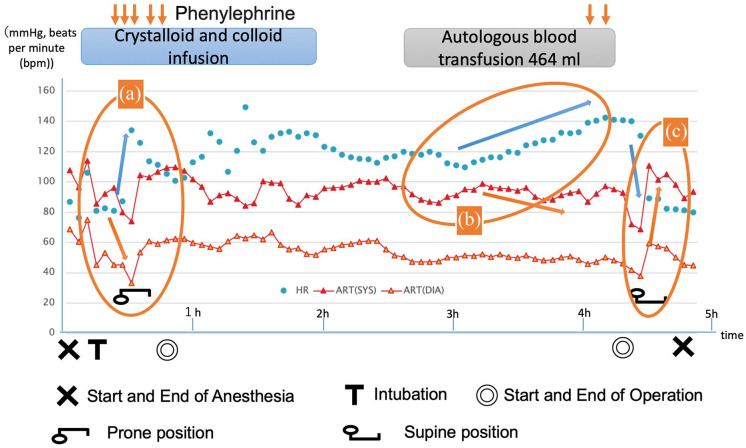
Hemodynamics may deteriorate during the perioperative period when performing posterior spinal fusion in patients with pectus excavatum and scoliosis. A 13-year-old teenager diagnosed with Marfan syndrome had thoracic scoliosis and pectus excavatum. Thoracic scoliosis was convex to the right, and a right ventricular inflow tract stenosis was observed due to compression induced by the depressed sternum. The patient underwent T3-L4 posterior spinal fusion surgery for scoliosis. Deterioration of hemodynamics was observed when the patient was placed in the prone position or when the thoracic spine was corrected to the left front. Postoperative computed tomography examination showed that the mediastinal space was narrowed due to the corrected thoracic spine. Special attention should be paid in the following cases: (1) severe pectus excavatum, (2) right ventricular inflow tract compression due to depressed sternum on the left side, (3) correction of the thoracic spine on the left front, (4) long-term surgery, and (5) risk of massive bleeding. In some cases, pectus excavatum surgery should be prioritized.
Keywords: Haller index; Marfan syndrome; Pectus excavatum; posterior spinal fusion; right ventricular inflow stenosis; scoliosis.
© The Author(s) 2022.
Conflict of interest statement
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



Similar articles
-
Progressive decrease in partial pressure of end-tidal CO2 during posterior spinal fusion surgery in a child with idiopathic scoliosis and pectus excavatum: a case report.BMC Musculoskelet Disord. 2024 Dec 18;25(1):1015. doi: 10.1186/s12891-024-08176-5. BMC Musculoskelet Disord. 2024. PMID: 39696291 Free PMC article.
-
Echocardiographic diagnosis of right ventricular inflow compression associated with pectus excavatum during spinal fusion in prone position.Congenit Heart Dis. 2009 May-Jun;4(3):193-5. doi: 10.1111/j.1747-0803.2008.00231.x. Congenit Heart Dis. 2009. PMID: 19489950
-
Evaluation of thoracic factors after scoliosis surgery in patients with both scoliosis and pectus excavatum.Eur Spine J. 2018 Feb;27(2):381-387. doi: 10.1007/s00586-016-4753-4. Epub 2016 Aug 27. Eur Spine J. 2018. PMID: 27568387
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
-
Pectus excavatum, kyphoscoliosis associated with thoracolumbar spinal stenosis: a rare case report and literature review.BMC Surg. 2022 Jul 11;22(1):266. doi: 10.1186/s12893-022-01716-7. BMC Surg. 2022. PMID: 35820858 Free PMC article. Review.
References
-
- Creswick HA, Stacey MW, Kelly RE, et al.. Family study of the inheritance of pectus excavatum. J Pediatr Surg 2006; 41: 1699–1703. - PubMed
-
- Waters P, Welch K, Micheli LJ, et al.. Scoliosis in children with pectus excavatum and pectus carinatum. J Pediatr Orthop 1989; 9(5): 551–556. - PubMed
-
- Hong JY, Suh SW, Park HJ, et al.. Correlations of adolescent idiopathic scoliosis and pectus excavatum. J Pediatr Orthop 2011; 31(8): 870–874. - PubMed
-
- Tauchi R, Kawakami N, Tsuji T, et al.. Evaluation of thoracic factors after scoliosis surgery in patients with both scoliosis and pectus excavatum. Eur Spine J 2018; 27(2): 381–387. - PubMed
-
- Ha HI, Seo JB, Lee SH, et al.. Imaging of Marfan syndrome: multisystemic manifestations. Radiographics 2007; 27(4): 989–1004. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
