

Exploration of the feasibility to combine patients with chronic obstructive pulmonary disease and chronic heart failure in self-management groups with focus on exercise self-efficacy
- PMID: 35575429
- PMCID: PMC9397432
- DOI: 10.1080/02813432.2022.2073961
Exploration of the feasibility to combine patients with chronic obstructive pulmonary disease and chronic heart failure in self-management groups with focus on exercise self-efficacy
Abstract
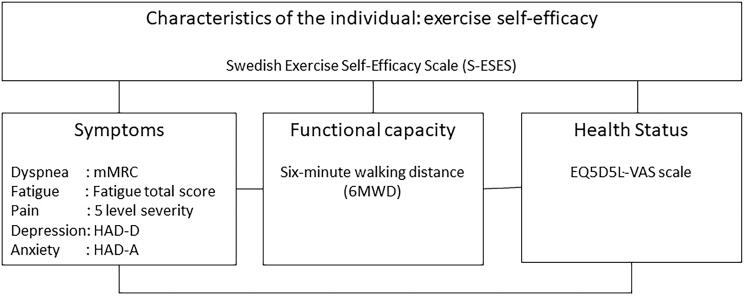
Objective: To compare the level of exercise self-efficacy, symptoms, functional capacity and health status and investigate the association between these variables in patients with chronic obstructive pulmonary disease (COPD) and chronic heart failure (CHF). Additionally, to investigate how diagnosis, symptoms and patient characteristics are associated with exercise self-efficacy in these patient groups.
Design: Cross-sectional study.
Setting: Primary care.
Subjects: Patients (n = 150) with COPD (n = 60), CHF (n = 60) and a double diagnosis (n = 30).
Main outcome measures: Swedish SCI Exercise Self-Efficacy score, modified Medical Research Council Dyspnea score (mMRC), fatigue score, pain severity score, Hospital Anxiety and Depression Scale, functional capacity measured as six-minute walking distance and health status measured by a Visual Analogue Scale.
Results: Levels of exercise self-efficacy, health status and symptoms were alike for patients with COPD and patients with CHF. Functional capacity was similar after correction for age. Associations with exercise self-efficacy were found for slight dyspnea (mMRC = 1) (R -4.45; 95% CI -8.41- -0.50), moderate dyspnea (mMRC = 2) (-6.60;-10.68- -2.52), severe dyspnea (mMRC ≥ 3) (-9.94; -15.07- -4.80), fatigue (-0.87;-1.41- -0.32), moderate pain (-3.87;-7.52- -0.21) and severe pain (-5.32;-10.13- -0.52), symptoms of depression (-0.98;-1.42- -0.55) and anxiety (-0.65;-0,10- -0.32), after adjustment for diagnosis, sex and age.
Conclusion and implications: Patients with COPD or CHF have similar levels of exercise self-efficacy, symptoms, functional capacity and health status. More severe symptoms are associated with lower levels of exercise self-efficacy regardless of diagnosis, sex and age. When forming self-management groups with a focus on exercise self-efficacy, it seems more relevant to consider level of symptoms than the specific diagnosis of COPD or CHF.Key pointsExercise training is an important part of self-management in patients with COPD and chronic heart failure (CHF). High exercise self-efficacy is required for optimal exercise training.Patients with COPD and CHF have similar symptoms and similar levels of exercise self-efficacy, functional capacity and health status.Not the diagnosis, but symptoms of dyspnea, fatigue, pain, depression and anxiety are important factors influencing exercise self-efficacy and need to be addressed.When forming self-management groups with a focus on exercise self-efficacy, it seems more relevant to consider the level of symptoms than the specific diagnosis of COPD or CHF.
Keywords: Pulmonary disease; chronic obstructive; exercise; feasibility studies; heart failure; self-efficacy; self-management.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Hawkins NM, Jhund PS, Simpson CR, et al. Primary care burden and treatment of patients with heart failure and chronic obstructive pulmonary disease in Scotland. Eur J Heart Fail. 2010;12(1):17–24. - PubMed
-
- Eide TB, Straand J, Björkelund C, et al. Differences in medical services in Nordic general practice: a comparative survey from the QUALICOPC study. Scand J Prim Health Care. 2017:1–10. - PubMed
-
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical