

Molecular diagnosis of ABMR with or without donor-specific antibody in kidney transplant biopsies: Differences in timing and intensity but similar mechanisms and outcomes
- PMID: 35575435
- PMCID: PMC9540308
- DOI: 10.1111/ajt.17092
Molecular diagnosis of ABMR with or without donor-specific antibody in kidney transplant biopsies: Differences in timing and intensity but similar mechanisms and outcomes
Abstract
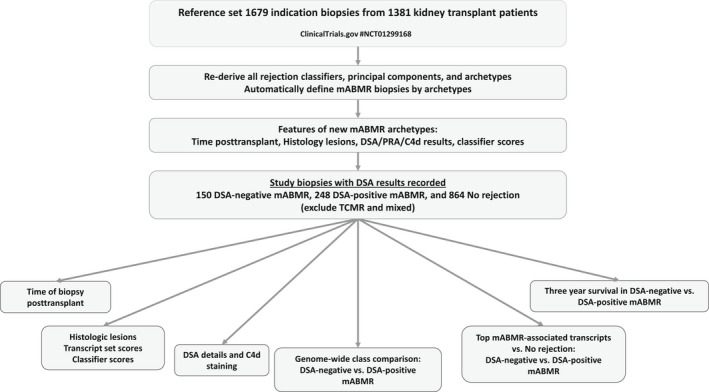
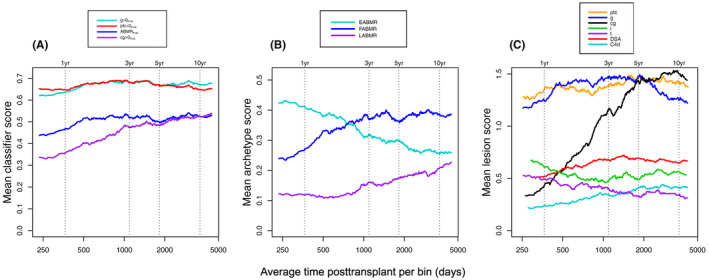
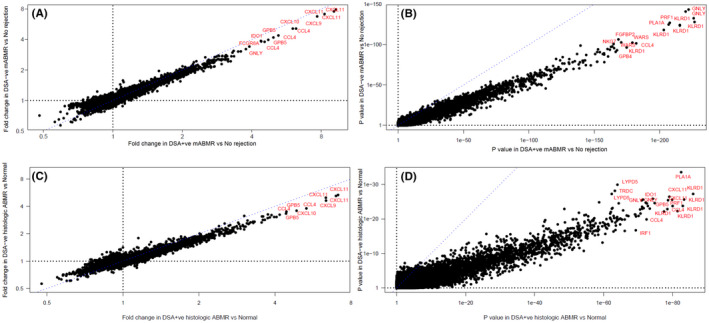
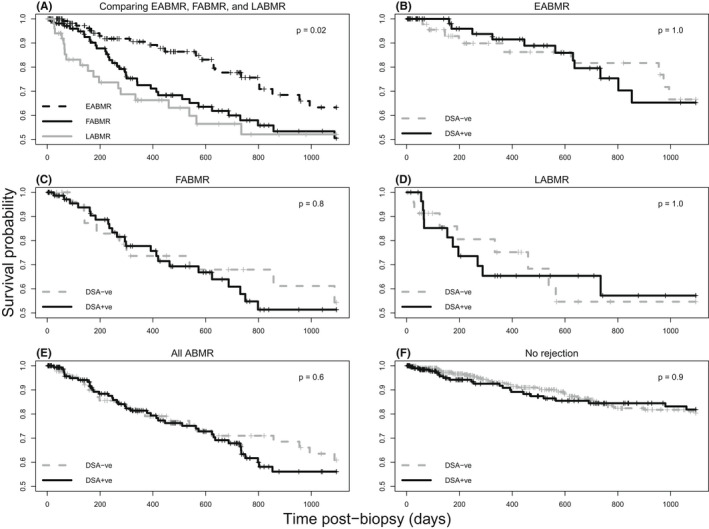
We studied the clinical, histologic, and molecular features distinguishing DSA-negative from DSA-positive molecularly defined antibody-mediated rejection (mABMR). We analyzed mABMR biopsies with available DSA assessments from the INTERCOMEX study: 148 DSA-negative versus 248 DSA-positive, compared with 864 no rejection (excluding TCMR and Mixed). DSA-positivity varied with mABMR stage: early-stage (EABMR) 56%; fully developed (FABMR) 70%; and late-stage (LABMR) 58%. DSA-negative patients with mABMR were usually sensitized, 60% being HLA antibody-positive. Compared with DSA-positive mABMR, DSA-negative mABMR was more often C4d-negative; earlier by 1.5 years (average 2.4 vs. 3.9 years); and had lower ABMR activity and earlier stage in molecular and histology features. However, the top ABMR-associated transcripts were identical in DSA-negative versus DSA-positive mABMR, for example, NK-associated (e.g., KLRD1 and GZMB) and IFNG-inducible (e.g., PLA1A). Genome-wide class comparison between DSA-negative and DSA-positive mABMR showed no significant differences in transcript expression except those related to lower intensity and earlier time of DSA-negative ABMR. Three-year graft loss in DSA-negative mABMR was the same as DSA-positive mABMR, even after adjusting for ABMR stage. Thus, compared with DSA-positive mABMR, DSA-negative mABMR is on average earlier, less active, and more often C4d-negative but has similar graft loss, and genome-wide analysis suggests that it involves the same mechanisms. SUMMARY SENTENCE: In 398 kidney transplant biopsies with molecular antibody-mediated rejection, the 150 DSA-negative cases are earlier, less intense, and mostly C4d-negative, but use identical molecular mechanisms and have the same risk of graft loss as the 248 DSA-positive cases.
Keywords: basic (laboratory) research/science; biopsy; kidney transplantation/nephrology; microarray/gene array; rejection; rejection: antibody-mediated (ABMR).
© 2022 The Authors. American Journal of Transplantation published by Wiley Periodicals LLC on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
Comment in
-
Microvascular inflammation: Gene expression changes do not necessarily reflect pathogenesis.Am J Transplant. 2022 Dec;22(12):3180-3181. doi: 10.1111/ajt.17136. Epub 2022 Jul 19. Am J Transplant. 2022. PMID: 35778949 No abstract available.
-
Letter to the Editor Re: Letter by Naesens et al. Microvascular inflammation: Gene expression changes do not necessarily reflect pathogenesis.Am J Transplant. 2022 Dec;22(12):3182-3183. doi: 10.1111/ajt.17169. Epub 2022 Aug 25. Am J Transplant. 2022. PMID: 35951469 No abstract available.
References
-
- Haas M, Loupy A, Lefaucheur C, et al. The Banff 2017 kidney meeting report: revised diagnostic criteria for chronic active T cell‐mediated rejection, antibody‐mediated rejection, and prospects for integrative endpoints for next‐generation clinical trials. Am J Transplant. 2018;18(2):293‐307. - PMC - PubMed
-
- Halloran PF, Wadgymar A, Ritchie S, Falk J, Solez K, Srinivasa NS. The significance of the anti‐class I antibody response. I. Clinical and pathologic features of anti‐class I‐mediated rejection. Transplantation. 1990;49(1):85‐91. - PubMed
-
- Bohmig GA, Exner M, Habicht A, et al. Capillary C4d deposition in kidney allografts: a specific marker of alloantibody‐dependent graft injury. J Am soc Nephrol. 2002;13(4):1091‐1099. - PubMed
-
- Regele H, Bohmig GA, Habicht A, et al. Capillary deposition of complement split product C4d in renal allografts is associated with basement membrane injury in peritubular and glomerular capillaries: a contribution of humoral immunity to chronic allograft rejection. J Am soc Nephrol. 2002;13(9):2371‐2380. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
