

The dose accumulation and the impact of deformable image registration on dose reporting parameters in a moving patient undergoing proton radiotherapy
- PMID: 35575586
- PMCID: PMC9122289
- DOI: 10.2478/raon-2022-0016
The dose accumulation and the impact of deformable image registration on dose reporting parameters in a moving patient undergoing proton radiotherapy
Abstract
Introduction: Potential changes in patient anatomy during proton radiotherapy may lead to a deviation of the delivered dose. A dose estimate can be computed through a deformable image registration (DIR) driven dose accumulation. The present study evaluates the accumulated dose uncertainties in a patient subject to an inadvertent breathing associated motion.
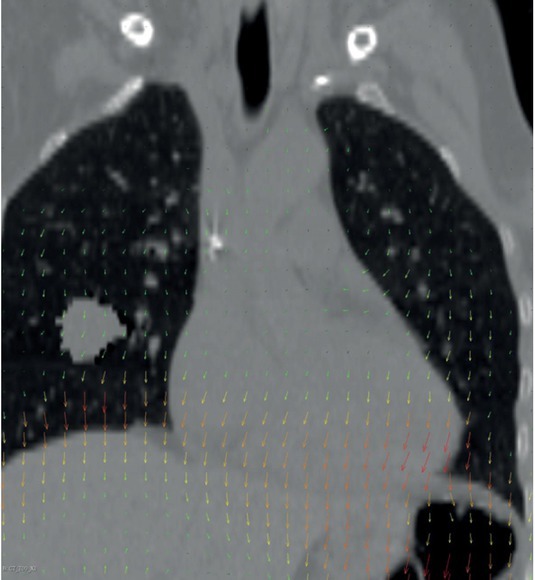
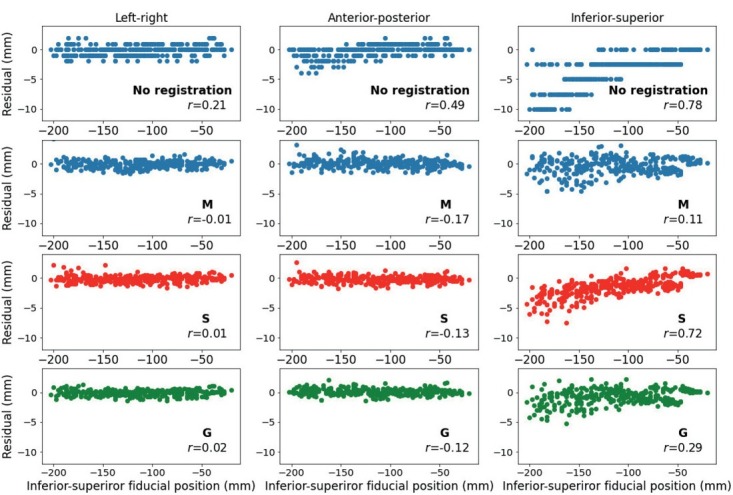
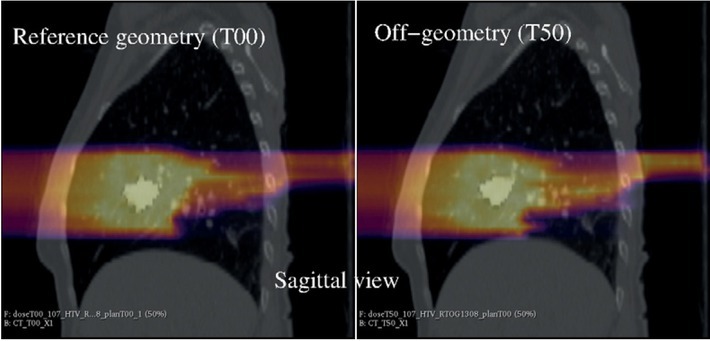
Materials and methods: A virtual lung tumour was inserted into a pair of single participant landmark annotated computed tomography images depicting opposite breathing phases, with the deep inspiration breath-hold the planning reference and the exhale the off-reference geometry. A novel Monte Carlo N-Particle, Version 6 (MCNP6) dose engine was developed, validated and used in treatment plan optimization. Three DIR methods were compared and used to transfer the exhale simulated dose to the reference geometry. Dose conformity and homogeneity measures from International Committee on Radioactivity Units and Measurements (ICRU) reports 78 and 83 were evaluated on simulated dose distributions registered with different DIR algorithms.
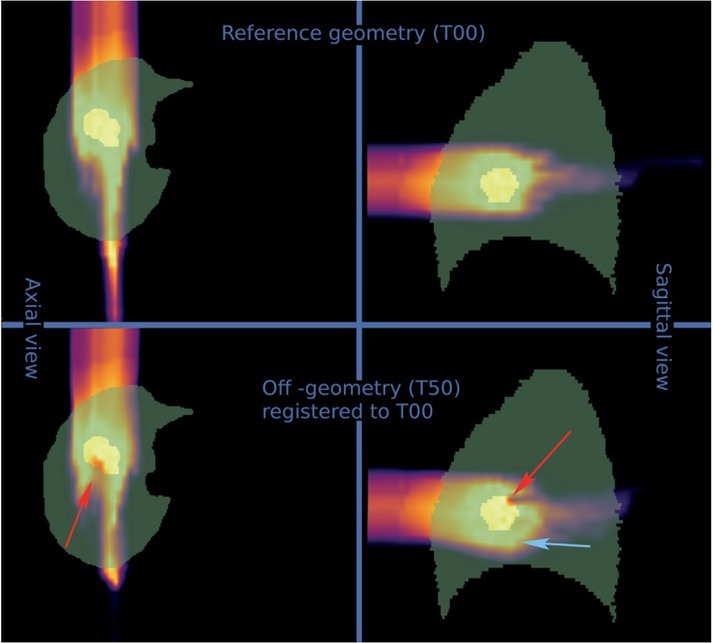
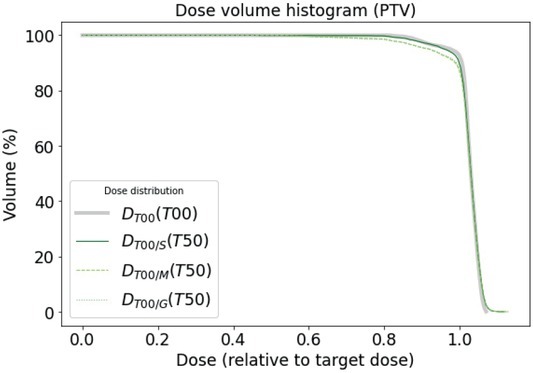
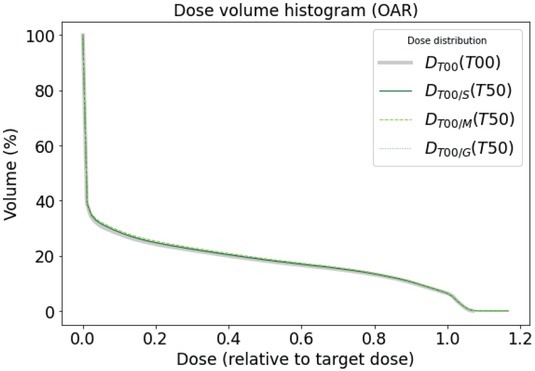
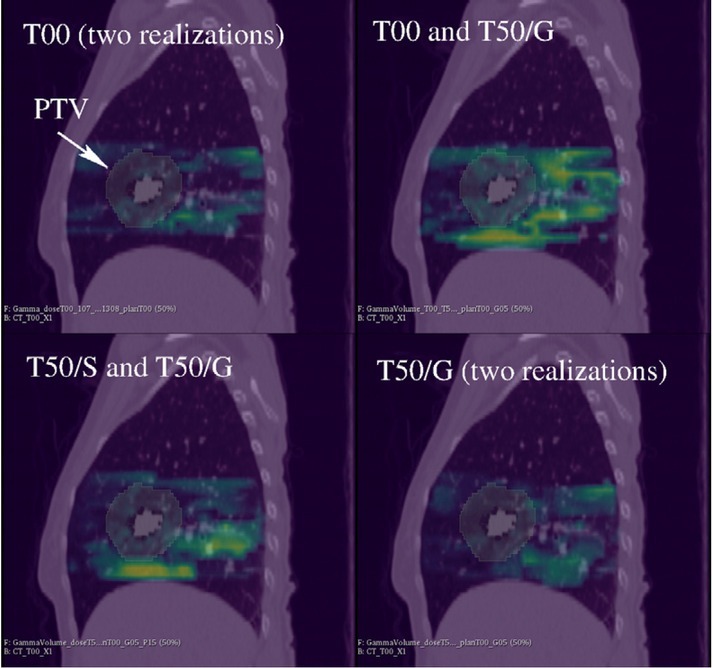
Results: The MCNP6 dose engine handled patient-like geometries in reasonable dose calculation times. All registration methods were able to align image associated landmarks to distances, comparable to voxel sizes. A moderate deterioration of ICRU measures was encountered in comparing doses in on and off-reference anatomy. There were statistically significant DIR driven differences in ICRU measures, particularly a 10% difference in the relative D98% for planning tumour volume and in the 3 mm/3% gamma passing rate.
Conclusions: T he dose accumulation over two anatomies resulted in a DIR driven uncertainty, important in reporting the associated ICRU measures for quality assurance.
Keywords: MCNP6; Monte-Carlo; adaptive therapy; dose distribution measurement; dose homogeneity; image registration; proton therapy.
© 2022 Gasper Razdevsek, Urban Simoncic, Luka Snoj, Andrej Studen, published by Sciendo.
Figures
References
-
- Liao Z, Lee JJ, Komaki R, Gomez DR, O’Reilly MS, Fossella FV. Bayesian adaptive randomization trial of passive scattering proton therapy and intensity-modulated photon radiotherapy for locally advanced non–small-cell lung cancer. J Clin Oncol. 2018;36:1813–22. doi: 10.1200/JCO.2017.74.0720. et al. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
