

Validation of the Pediatric Sequential Organ Failure Assessment Score and Evaluation of Third International Consensus Definitions for Sepsis and Septic Shock Definitions in the Pediatric Emergency Department
- PMID: 35575803
- PMCID: PMC9112137
- DOI: 10.1001/jamapediatrics.2022.1301
Validation of the Pediatric Sequential Organ Failure Assessment Score and Evaluation of Third International Consensus Definitions for Sepsis and Septic Shock Definitions in the Pediatric Emergency Department
Abstract
Importance: Pediatric sepsis definitions have evolved, and some have proposed using the measure used in adults to quantify organ dysfunction, a Sequential Organ Failure Assessment (SOFA) score of 2 or more in the setting of suspected infection. A pediatric adaptation of SOFA (pSOFA) showed excellent discrimination for mortality in critically ill children but has not been evaluated in an emergency department (ED) population.
Objective: To delineate test characteristics of the pSOFA score for predicting in-hospital mortality among (1) all patients and (2) patients with suspected infection treated in pediatric EDs.
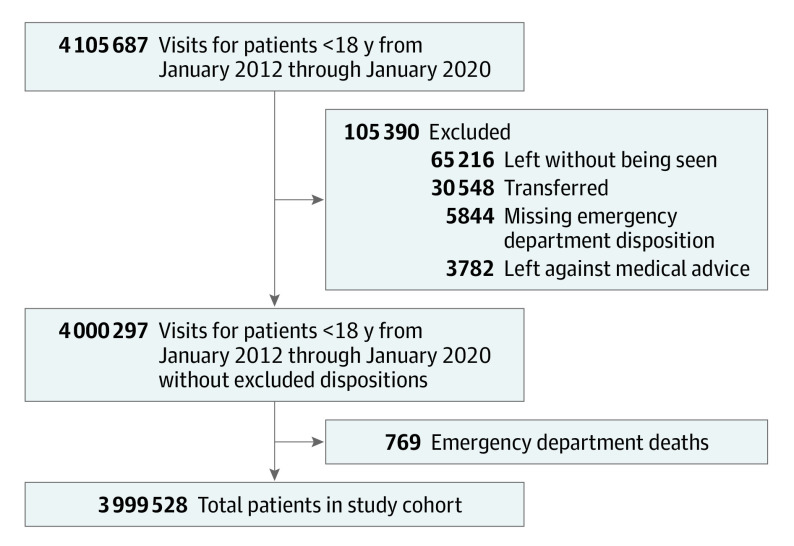
Design, setting, and participants: This retrospective cohort study took place from January 1, 2012, to January 31, 2020 in 9 US children's hospitals included in the Pediatric Emergency Care Applied Research Network (PECARN) Registry. The data was analyzed from February 1, 2020, to April 18, 2022. All ED visits for patients younger than 18 years were included.
Exposures: ED pSOFA score was assigned by summing maximum pSOFA organ dysfunction components during ED stay (each 0-4 points). In the subset with suspected infection, visit meeting criteria for sepsis (suspected infection with a pSOFA score of 2 or more) and septic shock (suspected infection with vasoactive infusion and serum lactate level >18.0 mg/dL) were identified.
Main outcomes and measures: Test characteristics of pSOFA scores of 2 or more during the ED stay for hospital mortality.
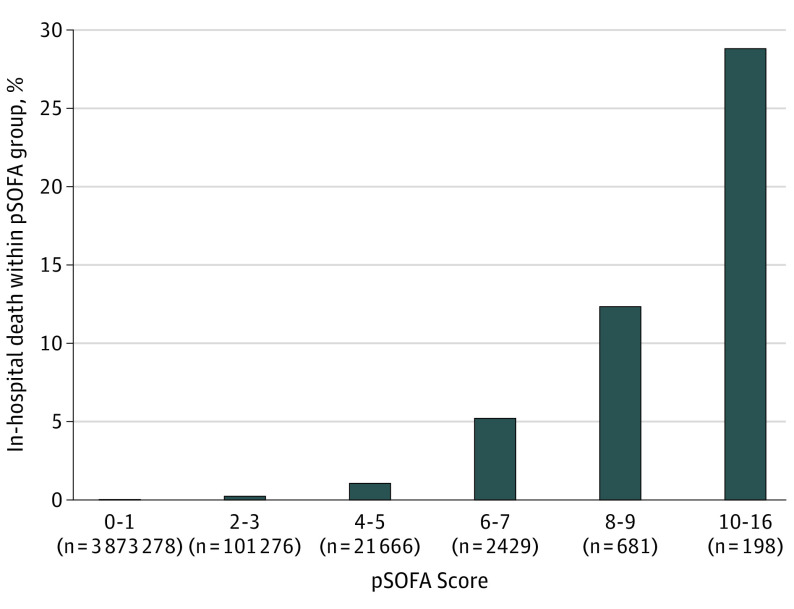
Results: A total of 3 999 528 (female, 47.3%) ED visits were included. pSOFA scores ranged from 0 to 16, with 126 250 visits (3.2%) having a pSOFA score of 2 or more. pSOFA scores of 2 or more had sensitivity of 0.65 (95% CI, 0.62-0.67) and specificity of 0.97 (95% CI, 0.97-0.97), with negative predictive value of 1.0 (95% CI, 1.00-1.00) in predicting hospital mortality. Of 642 868 patients with suspected infection (16.1%), 42 992 (6.7%) met criteria for sepsis, and 374 (0.1%) met criteria for septic shock. Hospital mortality rates for suspected infection (599 502), sepsis (42 992), and septic shock (374) were 0.0%, 0.9%, and 8.0%, respectively. The pSOFA score had similar discrimination for hospital mortality in all ED visits (area under receiver operating characteristic curve, 0.81; 95% CI, 0.79-0.82) and the subset with suspected infection (area under receiver operating characteristic curve, 0.82; 95% CI, 0.80-0.84).
Conclusions and relevance: In a large, multicenter study of pediatric ED visits, a pSOFA score of 2 or more was uncommon and associated with increased hospital mortality yet had poor sensitivity as a screening tool for hospital mortality. Conversely, children with a pSOFA score of 2 or less were at very low risk of death, with high specificity and negative predictive value. Among patients with suspected infection, patients with pSOFA-defined septic shock demonstrated the highest mortality.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
