

Association of the USPSTF Grade D Recommendation Against Prostate-Specific Antigen Screening With Prostate Cancer-Specific Mortality
- PMID: 35576008
- PMCID: PMC9112070
- DOI: 10.1001/jamanetworkopen.2022.11869
Association of the USPSTF Grade D Recommendation Against Prostate-Specific Antigen Screening With Prostate Cancer-Specific Mortality
Abstract
Importance: The 2012 US Preventive Services Task Force (USPSTF) Grade D recommendation against prostate-specific antigen (PSA) screening for all men has been controversial, with data documenting a shift to a higher stage of disease at diagnosis. The association between the Grade D recommendation and prostate cancer-specific mortality (PCSM) among contemporary cohorts, however, is unclear.
Objective: To evaluate PCSM rates between 1999 and 2019, comparing trends in rates before and after the change in the 2012 USPSTF screening guideline to assess its association with PCSM.
Exposure: The 2012 USPSTF Grade D recommendation against PSA screening for all men.
Design, setting, and participants: This cross-sectional study used Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research maintained by the National Center for Health Statistics to collect data on cause of death for all individuals who died of prostate cancer in the US from 1999 to 2019. Analysis was performed from January to August 2021.
Main outcomes and measures: Trends in PCSM rates were calculated from 1999 to 2012 and from 2014 to 2019, with a washout year of 2013, using linear regression, with year and binary indicator of pre-2013 and post-2013 status as interaction terms. Trends were further analyzed by age, race and ethnicity, urbanization category, and US Census region. Other measures included diagnosis of localized or metastatic prostate cancer and overall cancer mortality.
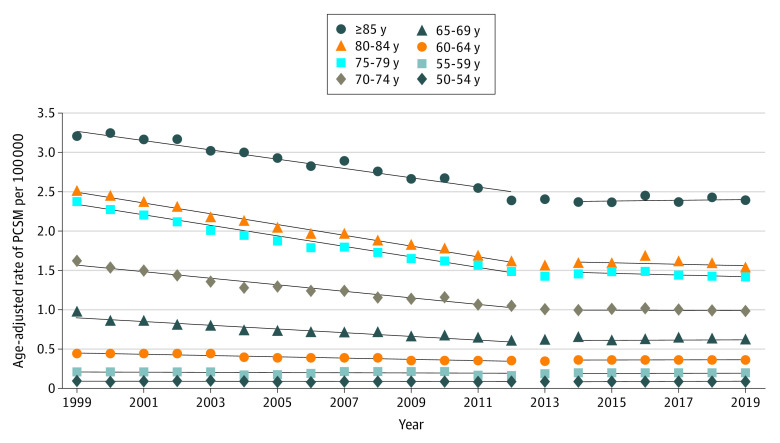
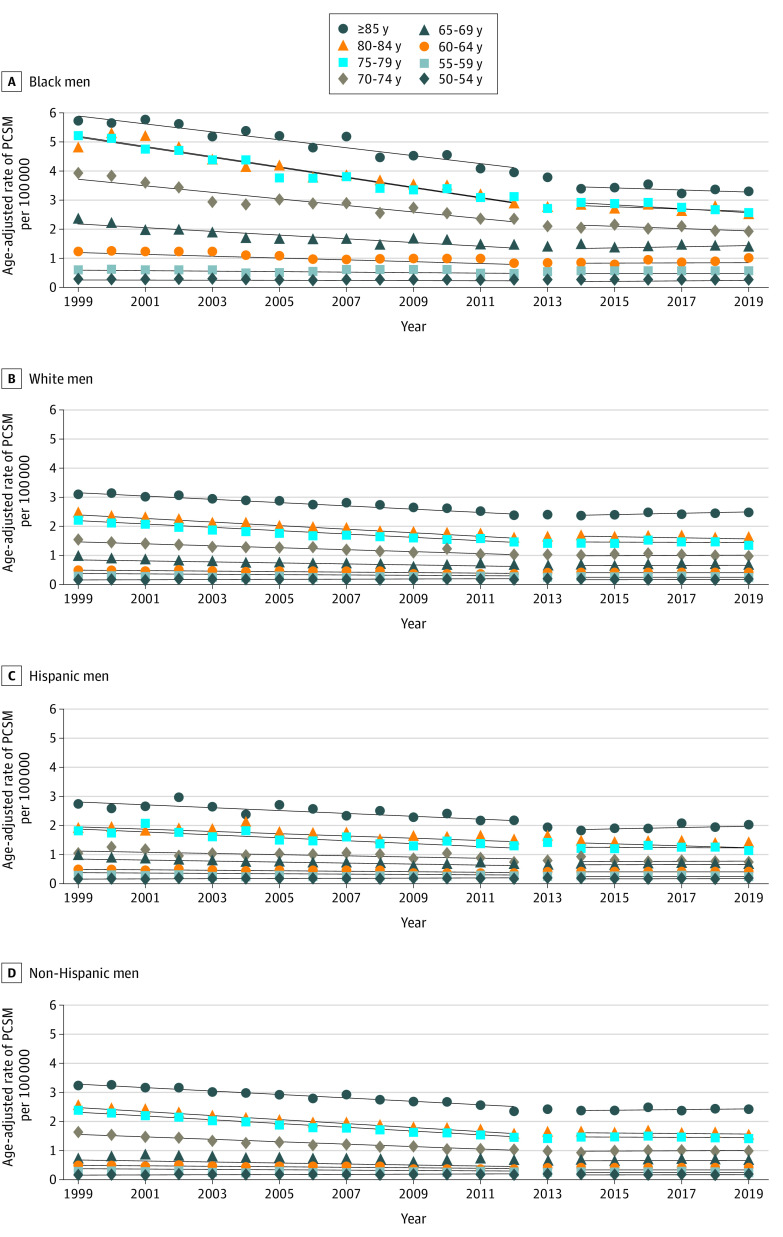
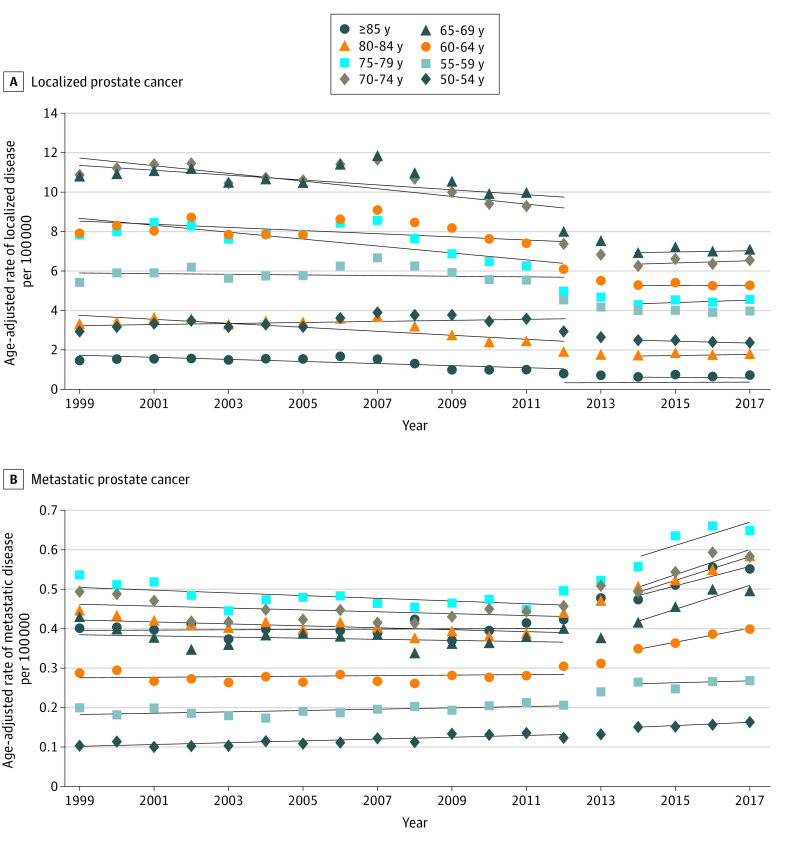
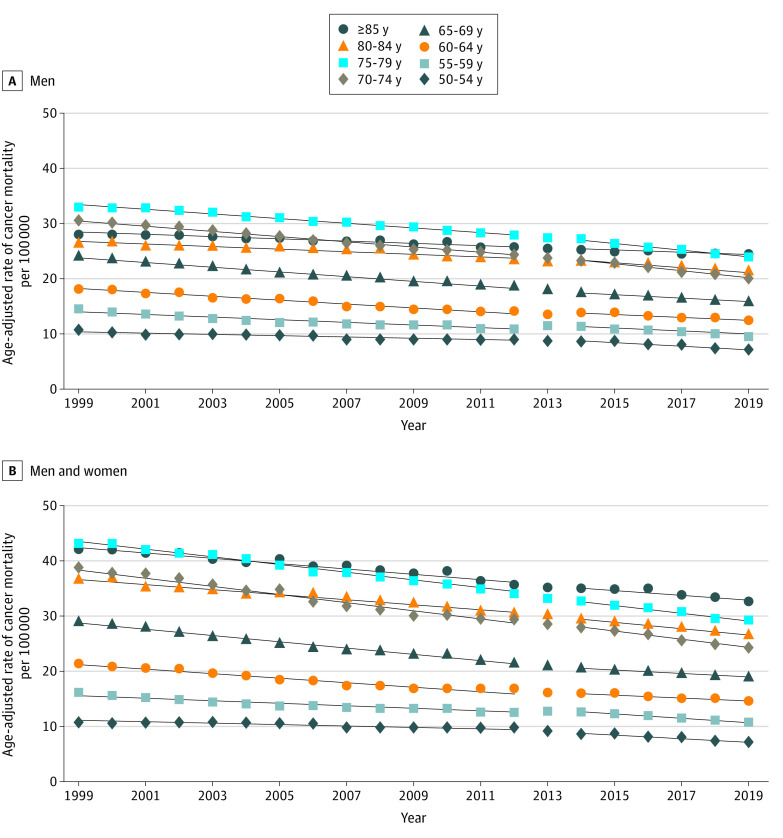
Results: A total of 618 095 patients died of prostate cancer in the US from 1999 to 2019. Age-adjusted PCSM decreased linearly at a rate of -0.273 per 100 000 population per year from 1999 to 2012 and stalled at a rate of -0.009 per 100 000 per year from 2014 to 2019 (P < .001). This finding was significant among men aged 60 years or older, especially among men aged 60 to 69 years, men aged 80 years or older, and among Black men. Men aged 60 to 64 years had a decreasing, age-adjusted PCSM rate of -0.0088 per 100 000 population per year prior to 2013 followed by an increasing rate of 0.0014 per 100 000 per year. Men aged 65 to 69 years had a decreasing, age-adjusted PCSM rate of -0.024 per 100 000 population per year prior to 2013 followed by an increasing rate of 0.0011 per 100 000 population per year. Men aged 80 years or older had the largest absolute difference between rates before and after 2013 compared with all other age groups, with a difference of 0.06 for men aged 80 to 84 years and 0.07 for men 85 aged years or older. Black men had a decreasing, age-adjusted PCSM rate of -0.700 per 100 000 population per year prior to 2013 followed by a flattened rate of -0.091 per 100 000 population per year. Changes were observed across races and ethnicities, urbanization categories, and US Census regions and were accompanied by increased diagnoses of metastatic disease, which are inconsistent with mortality trends across all malignant neoplasms.
Conclusions and relevance: This cross-sectional study using comprehensive PCSM data through 2019 demonstrated decreasing PCSM rates that flattened or increased after the 2012 USPSTF Grade D recommendation, suggesting that decreased PSA screening may be a factor associated with this change. This change was seen across ages, races and ethnicities, urbanization categories, and US Census regions. The updated 2018 USPSTF guideline supporting shared decision-making may reverse these trends in the coming years.
Conflict of interest statement
Figures
References
-
- National Cancer Institute . Cancer stat facts: prostate cancer. Accessed March 30, 2021. https://seer.cancer.gov/statfacts/html/prost.html
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
