

A Revised Markov Model Evaluating Oophorectomy at the Time of Hysterectomy for Benign Indication: Age 65 Years Revisited
- PMID: 35576331
- PMCID: PMC9015029
- DOI: 10.1097/AOG.0000000000004732
A Revised Markov Model Evaluating Oophorectomy at the Time of Hysterectomy for Benign Indication: Age 65 Years Revisited
Abstract
Objective: To perform an updated Markov modeling to assess the optimal age for bilateral salpingo-oophorectomy (BSO) at the time of hysterectomy for benign indication.
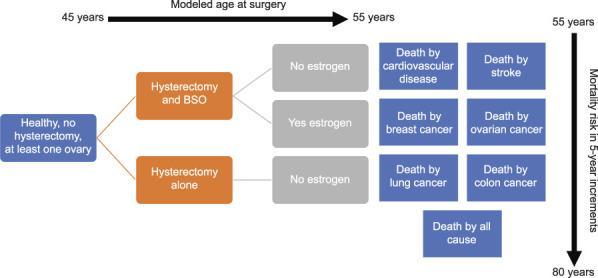
Methods: We performed a literature review that assessed hazard ratios (HRs) for mortality by disease, age, hysterectomy with or without BSO, and estrogen therapy use. Base mortality rates were derived from national vital statistics data. A Markov model from reported HRs predicted the proportion of the population staying alive to age 80 years by 1-year and 5-year age groups at time of surgery, from age 45 to 55 years. Those younger than age 50 years were modeled as either taking postoperative estrogen or not; those 50 and older were modeled as not receiving estrogen. Computations were performed with R 3.5.1, using Bayesian integration for HR uncertainty.
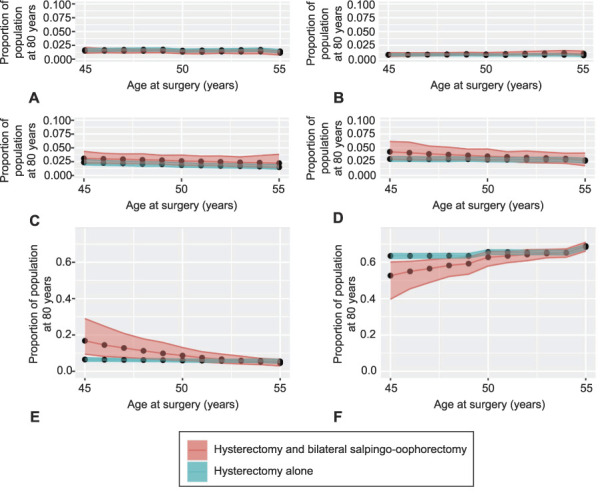
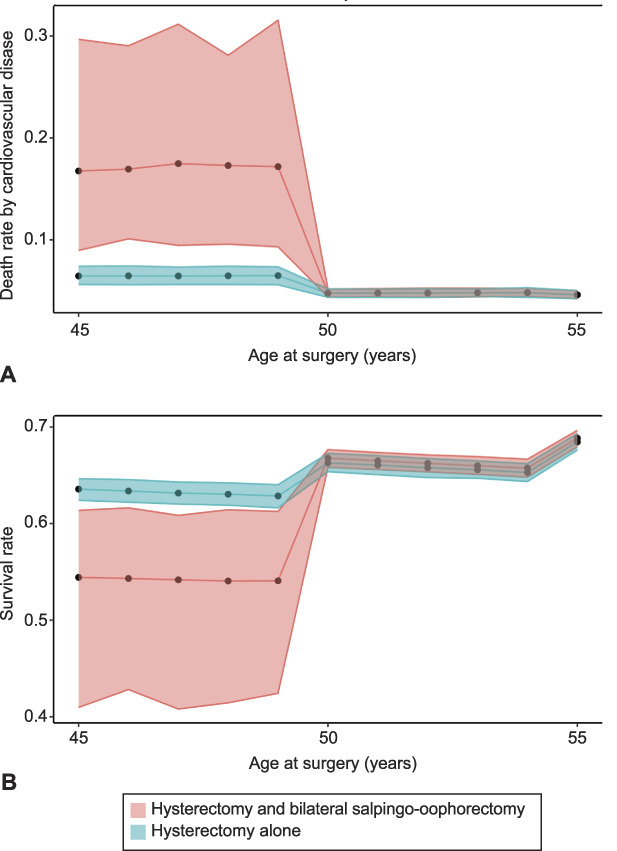
Results: Performing salpingo-oophorectomy before age 50 years for those not taking estrogen yields a lower survival proportion to age 80 years than hysterectomy alone before age 50 years (52.8% [Bayesian CI 40.7-59.7] vs 63.5% [Bayesian CI 62.2-64.9]). At or after age 50 years, there were similar proportions of those living to age 80 years with hysterectomy alone (66.4%, Bayesian CI 65.0-67.6) compared with concurrent salpingo-oophorectomy (66.9%, Bayesian CI 64.4-69.0). Importantly, those taking estrogen when salpingo-oophorectomy was performed before age 50 years had similar proportions of cardiovascular disease, stroke, and people living to age 80 years as those undergoing hysterectomy alone or those undergoing hysterectomy and salpingo-oophorectomy at age 50 years and older.
Conclusion: This updated Markov model argues for the consideration of concurrent salpingo-oophorectomy for patients who are undergoing hysterectomy at age 50 and older and suggests that initiating estrogen in those who need salpingo-oophorectomy before age 50 years mitigates increased mortality risk.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Financial Disclosure The authors did not report any potential conflicts of interest.
Figures
Comment in
-
The Swinging Pendulum: Elective Oophorectomy at the Time of Hysterectomy.Obstet Gynecol. 2022 May 1;139(5):721-723. doi: 10.1097/AOG.0000000000004776. Epub 2022 Apr 5. Obstet Gynecol. 2022. PMID: 35576329 No abstract available.
-
A Revised Markov Model Evaluating Oophorectomy at the Time of Hysterectomy for Benign Indication: Age 65 Years Revisited.Obstet Gynecol. 2022 Sep 1;140(3):520-521. doi: 10.1097/AOG.0000000000004912. Obstet Gynecol. 2022. PMID: 36356241 No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
