

Intraperitoneal drain placement and outcomes after elective colorectal surgery: international matched, prospective, cohort study
- PMID: 35576382
- PMCID: PMC10364732
- DOI: 10.1093/bjs/znac069
Intraperitoneal drain placement and outcomes after elective colorectal surgery: international matched, prospective, cohort study
Abstract
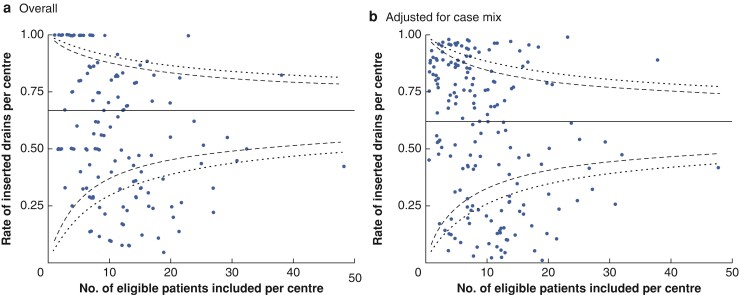
Background: Many surgeons routinely place intraperitoneal drains after elective colorectal surgery. However, enhanced recovery after surgery guidelines recommend against their routine use owing to a lack of clear clinical benefit. This study aimed to describe international variation in intraperitoneal drain placement and the safety of this practice.
Methods: COMPASS (COMPlicAted intra-abdominal collectionS after colorectal Surgery) was a prospective, international, cohort study which enrolled consecutive adults undergoing elective colorectal surgery (February to March 2020). The primary outcome was the rate of intraperitoneal drain placement. Secondary outcomes included: rate and time to diagnosis of postoperative intraperitoneal collections; rate of surgical site infections (SSIs); time to discharge; and 30-day major postoperative complications (Clavien-Dindo grade at least III). After propensity score matching, multivariable logistic regression and Cox proportional hazards regression were used to estimate the independent association of the secondary outcomes with drain placement.
Results: Overall, 1805 patients from 22 countries were included (798 women, 44.2 per cent; median age 67.0 years). The drain insertion rate was 51.9 per cent (937 patients). After matching, drains were not associated with reduced rates (odds ratio (OR) 1.33, 95 per cent c.i. 0.79 to 2.23; P = 0.287) or earlier detection (hazard ratio (HR) 0.87, 0.33 to 2.31; P = 0.780) of collections. Although not associated with worse major postoperative complications (OR 1.09, 0.68 to 1.75; P = 0.709), drains were associated with delayed hospital discharge (HR 0.58, 0.52 to 0.66; P < 0.001) and an increased risk of SSIs (OR 2.47, 1.50 to 4.05; P < 0.001).
Conclusion: Intraperitoneal drain placement after elective colorectal surgery is not associated with earlier detection of postoperative collections, but prolongs hospital stay and increases SSI risk.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures


References
-
- Memon MA, Memon MI, Donohue JH. Abdominal drains: a brief historical review. Ir Med J 2001;94:164–166 - PubMed
-
- Mujagic E, Zeindler J, Coslovsky M, Hoffmann H, Soysal SD, Mechera R et al. The association of surgical drains with surgical site infections—a prospective observational study. Am J Surg 2019;217:17–23 - PubMed
-
- Findik UY, Topcu SY, Vatansever O. Effects of drains on pain. Comfort and anxiety in patients undergone surgery. Int J Caring Sci 2013;6:412–419
