

A phase 1 dose escalation study of the pyruvate kinase activator mitapivat (AG-348) in sickle cell disease
- PMID: 35576529
- PMCID: PMC9837441
- DOI: 10.1182/blood.2022015403
A phase 1 dose escalation study of the pyruvate kinase activator mitapivat (AG-348) in sickle cell disease
Abstract
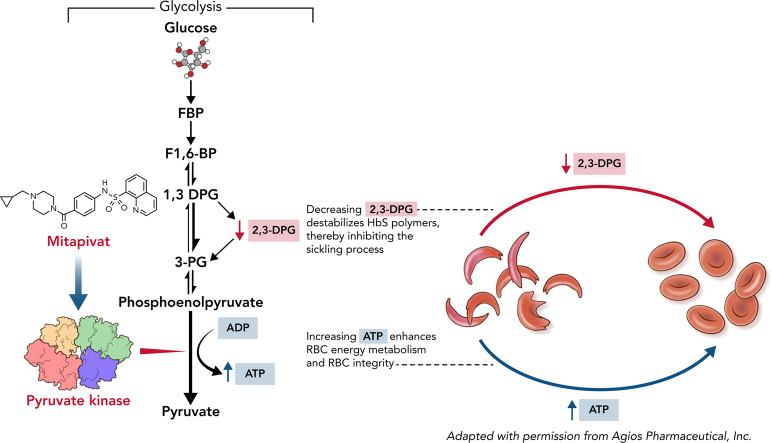
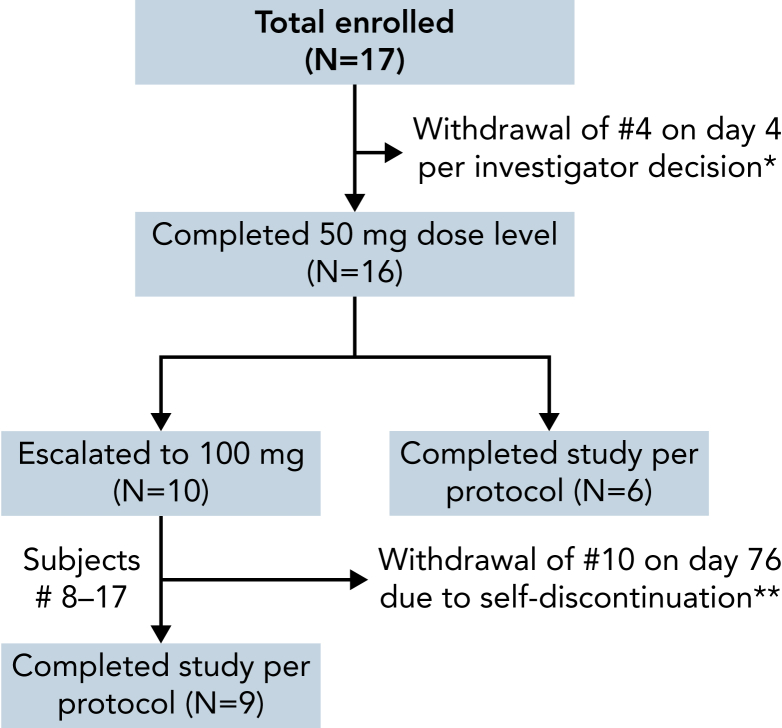
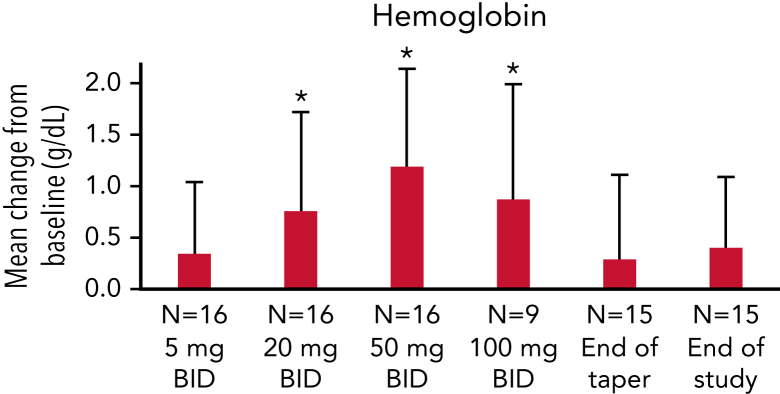
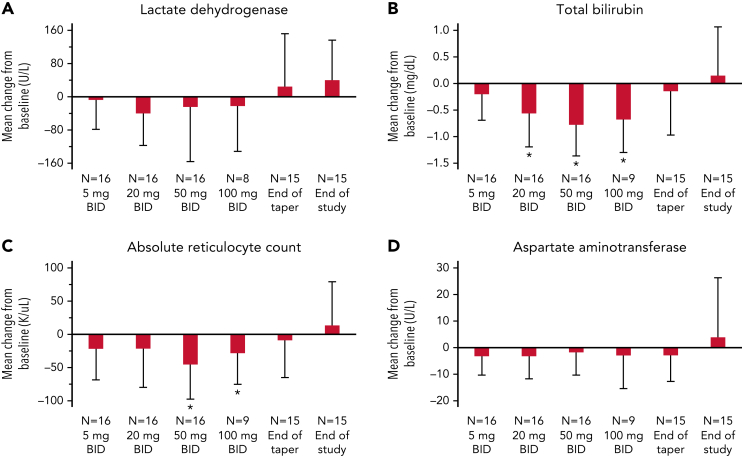
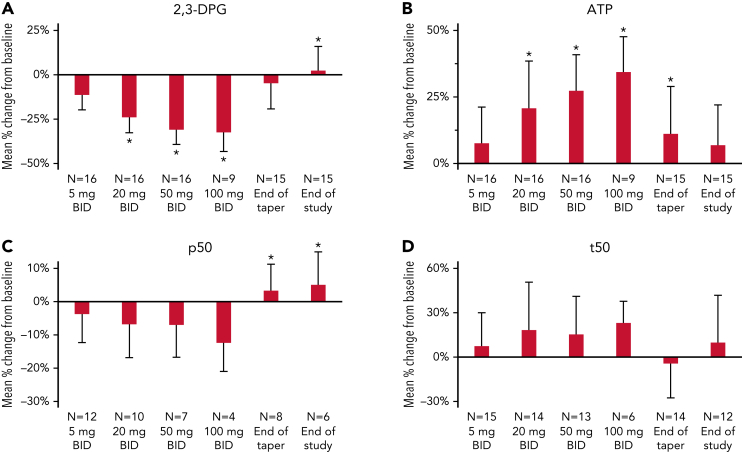
Polymerization of deoxygenated hemoglobin S underlies the pathophysiology of sickle cell disease (SCD). In activating red blood cell pyruvate kinase and glycolysis, mitapivat (AG-348) increases adenosine triphosphate (ATP) levels and decreases the 2,3-diphosphoglycerate (2,3-DPG) concentration, an upstream precursor in glycolysis. Both changes have therapeutic potential for patients with SCD. Here, we evaluated the safety and tolerability of multiple ascending doses of mitapivat in adults with SCD with no recent blood transfusions or changes in hydroxyurea or l-glutamine therapy. Seventeen subjects were enrolled; 1 subject was withdrawn shortly after starting the study. Sixteen subjects completed 3 ascending dose levels of mitapivat (5, 20, and 50 mg, twice daily [BID]) for 2 weeks each; following a protocol amendment, the dose was escalated to 100 mg BID in 9 subjects. Mitapivat was well tolerated at all dose levels, with the most common treatment-emergent adverse events (AEs) being insomnia, headache, and hypertension. Six serious AEs (SAEs) included 4 vaso-occlusive crises (VOCs), non-VOC-related shoulder pain, and a preexisting pulmonary embolism. Two VOCs occurred during drug taper and were possibly drug related; no other SAEs were drug related. Mean hemoglobin increase at the 50 mg BID dose level was 1.2 g/dL, with 9 of 16 (56.3%) patients achieving a hemoglobin response of a ≥1 g/dL increase compared with baseline. Mean reductions in hemolytic markers and dose-dependent decreases in 2,3-DPG and increases in ATP were also observed. This study provides proof of concept that mitapivat has disease-modifying potential in patients with SCD. This trial was registered at www.clinicaltrials.gov as #NCT04000165.
Conflict of interest statement
Conflict-of-interest disclosure: V.I., H.M., C.K., L.D., P.A.K., and P.H. are employed by and are stockholders in Agios. H.M. and P.H. are stockholders in Bristol-Myers Squibb. V.I. is a stockholder in Novartis. The remaining authors declare no competing financial interests.
Figures
Comment in
-
RBC, heal thyself: PK activators in SCD.Blood. 2022 Nov 10;140(19):2005-2006. doi: 10.1182/blood.2022016930. Blood. 2022. PMID: 36355466 No abstract available.
References
-
- Xu JZ, Conrey A, Frey I, et al. Phase 1 multiple ascending dose study of safety, tolerability, and pharmacokinetics/pharmacodynamics of mitapivat (AG-348) in subjects with sickle cell disease. Blood. 2020;136(suppl 1):21–22.
-
- Xu JZ, Conrey A, Frey I, et al. Mitapivat (AG-348) demonstrates safety, tolerability, and improvements in anemia, hemolysis, oxygen affinity, and hemoglobin s polymerization kinetics in adults with sickle cell disease: a phase 1 dose escalation study. Blood. 2021;138(suppl 1):10.
-
- Barabino GA, Platt MO, Kaul DK. Sickle cell biomechanics. Annu Rev Biomed Eng. 2010;12(1):345–367. - PubMed
