

Couples-based interventions and postpartum contraceptive uptake: A systematic review
- PMID: 35577147
- PMCID: PMC9968552
- DOI: 10.1016/j.contraception.2022.05.001
Couples-based interventions and postpartum contraceptive uptake: A systematic review
Abstract
Objective: Systematically review the existing evidence about couples-based interventions and postpartum contraceptive uptake and generate recommendations for future research.
Data sources: PubMed, Web of Science, PsycINFO, Embase, and CINAHL through June 7, 2021.
Study selection and data extraction: Studies with a couples-based intervention assessing postpartum contraceptive uptake. Two independent reviewers screened studies, extracted data, and assessed risk of bias with RoB-2 (Cochrane Risk of Bias 2) for randomized and ROBINS-I (Risk of Bias in Non-Randomized Studies - Interventions) for observational studies. Data were synthesized in tables, figures, and a narrative review.
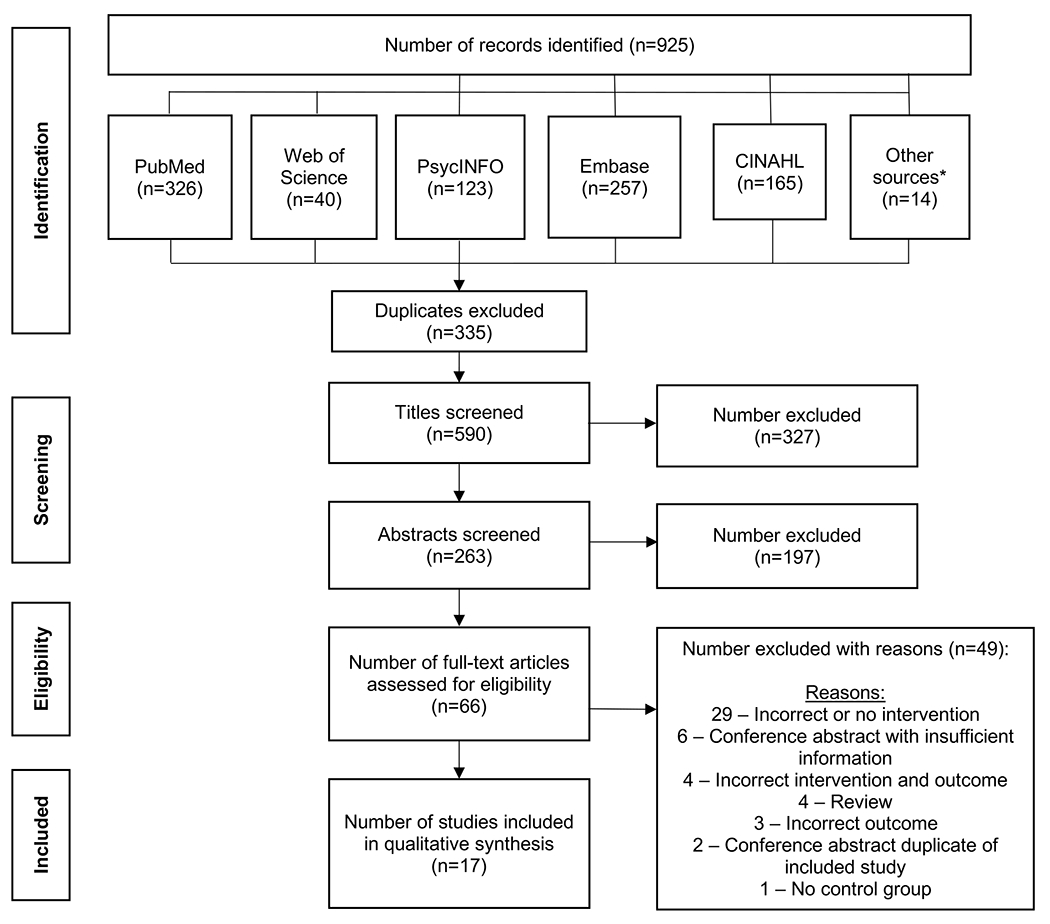
Results: A total of 925 papers were identified, 66 underwent full text review, and 17 articles, which included 18 studies - 16 randomized, 2 observational - were included. The lack of intervention and outcome homogeneity precluded meta-analysis and isolating the effect of partner involvement. Four studies were partner-required, where partner involvement was a required component of the intervention, and 14 were partner-optional. Unadjusted risk differences ranged from 0.01 to 0.51 in favor of couples-based interventions increasing postpartum contraceptive uptake versus standard of care. Bias assessment of the 16 randomized studies classified 8, 3, and 5 studies as at a high, some concern, and low risk of bias. Common sources of bias included intervention non-adherence and missing outcome data. One observational study was at a high and the other at a low risk of bias.
Conclusions: Future studies that assess couples-based interventions must clearly define and measure how partners are involved in the intervention and assess how intervention adherence impacts postpartum contraceptive uptake.
Keywords: Contraception; Postpartum period; Sexual partners; Spouses; Systematic review.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures


References
-
- World Health Organization. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland: 13-15 June 2005 2007.
-
- American College of Nurse-Midwives and the National Association of Nurse Practitioners in Women’s Health, American College of Obstetricians and Gynecologists and the Society for Maternal–Fetal Medicine, Louis JM, Bryant A, Ramos D, Stuebe A, et al. Interpregnancy Care. Am J Obstet Gynecol 2019;220:B2–18. 10.1016/j.ajog.2018.11.1098. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
