

Cost-Utility Analysis Compared Between Radiotherapy Alone and Combined Surgery and Radiotherapy for Symptomatic Spinal Metastases in Thailand
- PMID: 35577341
- PMCID: PMC9260553
- DOI: 10.14245/ns.2142948.474
Cost-Utility Analysis Compared Between Radiotherapy Alone and Combined Surgery and Radiotherapy for Symptomatic Spinal Metastases in Thailand
Abstract
Objective: To investigate the patient quality of life and cost-utility compared between radiotherapy alone and combined surgery and radiotherapy for spinal metastasis (SM) in Thailand.
Methods: Patients with SM with an indication for surgery during 2018-2020 were prospectively recruited. Patients were assigned to either the combination surgery and radiotherapy group or the radiotherapy alone group. Quality of life was assessed by EuroQol-5D-5L (EQ-5D-5L) questionnaire, and relevant healthcare costs were collected pretreatment, and at 3-month and 6-month posttreatment. Total lifetime cost and quality-adjusted life-years (QALYs) were estimated for each group.
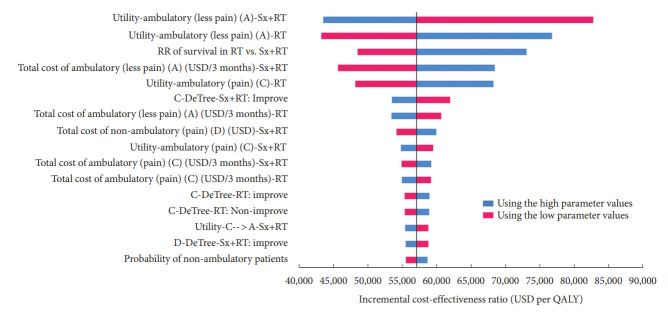
Results: Twenty-four SM patients (18 females, 6 males) were included. Of those, 12 patients underwent combination treatment, and 12 underwent radiotherapy alone. At 6-month posttreatment, 10 patients in the surgery group, and 11 patients in the nonsurgery group remained alive for a survival rate of 83.3% and 91.7%, retrospectively. At 6-month posttreatment, the mean utility in the combination treatment group was significantly better than in the radiotherapy alone group (0.804 ± 0.264 vs. 0.518 ± 0.282, respectively; p = 0.011). Total lifetime costs were 59,863.14 United States dollar (USD) in the combination treatment group and 24,526.97 USD in the radiation-only group. The incremental cost-effectiveness ratio using 6-month follow-up data was 57,074.01 USD per QALY gained.
Conclusion: Surgical treatment combined with radiotherapy to treat SM significantly improved patient quality of life compared to radiotherapy alone during the 6-month posttreatment period. However, combination treatment was found not to be cost-effective compared to radiotherapy alone for SM at the Thailand willingness-to-pay threshold of 5,113 USD/QALY.
Keywords: Combined surgery and radiotherapy; Cost-utility; Patient quality of life; Radiotherapy alone; Spinal metastasis.
Conflict of interest statement
The authors have nothing to disclose.
Figures


References
-
- de Ruiter GC, Nogarede CO, Wolfs JF, et al. Quality of life after different surgical procedures for the treatment of spinal metastases: results of a single-center prospective case series. Neurosurg Focus. 2017;42:E17. - PubMed
-
- Miyazaki S, Kakutani K, Sakai Y, et al. Quality of life and cost-utility of surgical treatment for patients with spinal metastases: prospective cohort study. Int Orthop. 2017;41:1265–71. - PubMed
-
- Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366:643–8. - PubMed
-
- Versteeg AL, Sahgal A, Rhines LD, et al. Health related quality of life outcomes following surgery and/or radiation for patients with potentially unstable spinal metastases. Spine J. 2021;21:492–9. - PubMed
LinkOut - more resources
Full Text Sources
