

The risk of death or unplanned readmission after discharge from a COVID-19 hospitalization in Alberta and Ontario
- PMID: 35577377
- PMCID: PMC9438727
- DOI: 10.1503/cmaj.220272
The risk of death or unplanned readmission after discharge from a COVID-19 hospitalization in Alberta and Ontario
Abstract
Background: The frequency of readmissions after COVID-19 hospitalizations is uncertain, as is whether current readmission prediction equations are useful for discharge risk stratification of COVID-19 survivors or for comparing among hospitals. We sought to determine the frequency and predictors of death or unplanned readmission after a COVID-19 hospital discharge.
Methods: We conducted a retrospective cohort study of all adults (≥ 18 yr) who were discharged alive from hospital after a nonpsychiatric, nonobstetric, acute care admission for COVID-19 between Jan. 1, 2020, and Sept. 30, 2021, in Alberta and Ontario.
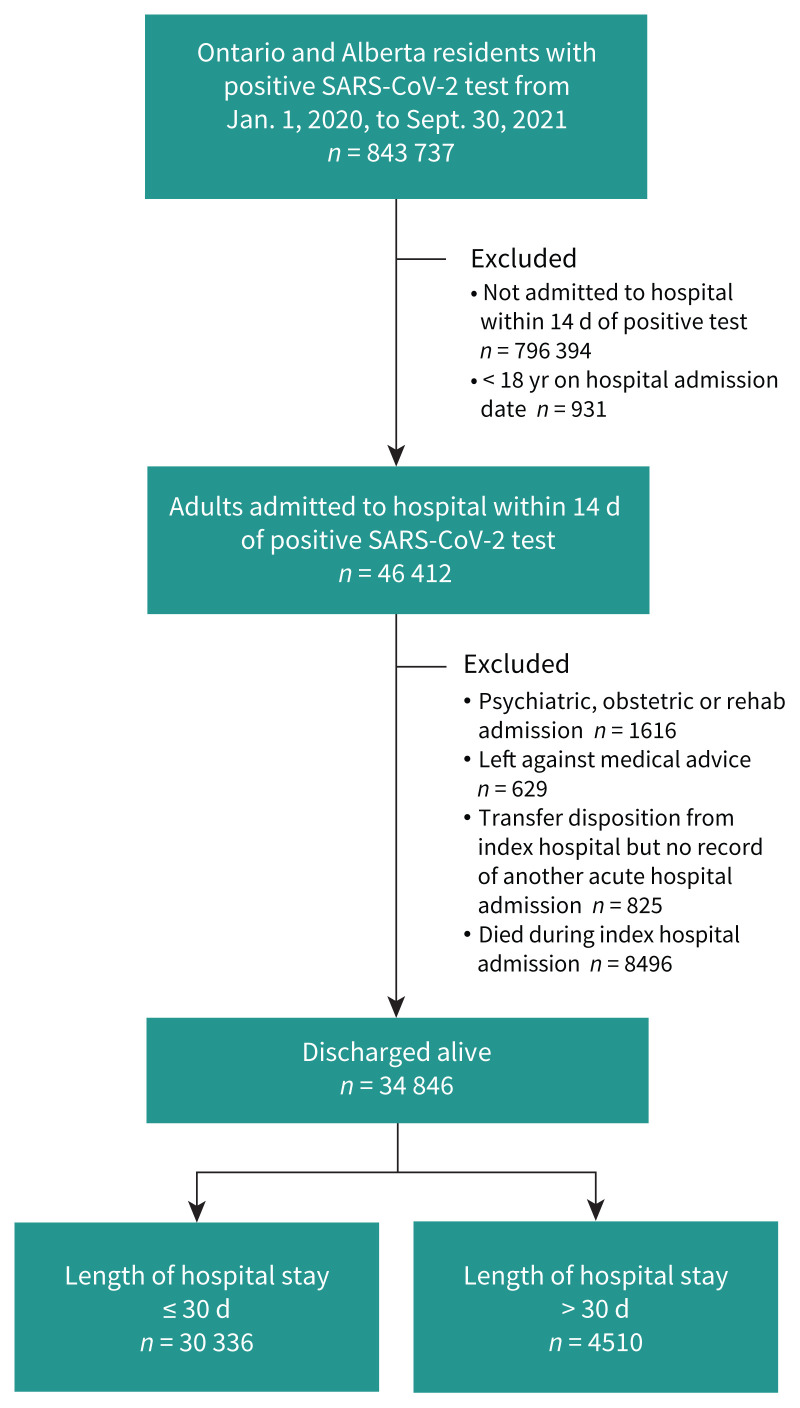
Results: Of 843 737 individuals who tested positive for SARS-CoV-2 by reverse transcription polymerase chain reaction during the study period, 46 412 (5.5%) were adults admitted to hospital within 14 days of their positive test. Of these, 8496 died in hospital and 34 846 were discharged alive (30 336 discharged after an index admission of ≤ 30 d and 4510 discharged after an admission > 30 d). One in 9 discharged patients died or were readmitted within 30 days after discharge (3173 [10.5%] of those with stay ≤ 30 d and 579 [12.8%] of those with stay > 30 d). The LACE score (length of stay, acuity, Charlson Comorbidity Index and number of emergency visits in previous 6 months) for predicting urgent readmission or death within 30 days had a c-statistic of 0.60 in Alberta and 0.61 in Ontario; inclusion of sex, discharge locale, deprivation index and teaching hospital status in the model improved the c-statistic to 0.73.
Interpretation: Death or readmission after discharge from a COVID-19 hospitalization is common and had a similar frequency in Alberta and Ontario. Risk stratification and interinstitutional comparisons of outcomes after hospital admission for COVID-19 should include sex, discharge locale and socioeconomic measures, in addition to the LACE variables.
© 2022 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Kieran Quinn has a grant from the Canadian Institutes of Health Research (CIHR) for a study of long COVID-19, and reports stock in BioNTech and Merck. Amol Verma holds research grants from CIHR, the Canadian Frailty Network, the Digital Research Alliance of Canada, the St. Michael’s Hospital Association, the St. Michael’s Hospital Foundation and the University of Toronto to support research related to COVID-19. He is the provincial clinical lead for quality improvement in general internal medicine with Ontario Health. Jacob Udell reports grants from Amgen, Bayer, Boehringer-Ingelheim, Novartis and Sanofi. Amy Yu holds a new investigator award from the Heart and Stroke Foundation of Canada and an AFP Innovation award, and grants from the CIHR, Health Data Research Network Canada and Academic Health Sciences Centres of Ontario. Fahad Razak receives a salary from Ontario Health, is assistant director of the Ontario COVID-19 Science Advisory Table and has a salary award from the Physicians’ Services Incorporated (PSI) Foundation.
References
-
- Atalla E, Kalligeros M, Giampaolo G, et al. . Readmissions among patients with COVID-19. Int J Clin Pract 2021;75:e13700. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous