

Anti-CSF-1R emactuzumab in combination with anti-PD-L1 atezolizumab in advanced solid tumor patients naïve or experienced for immune checkpoint blockade
- PMID: 35577503
- PMCID: PMC9114963
- DOI: 10.1136/jitc-2021-004076
Anti-CSF-1R emactuzumab in combination with anti-PD-L1 atezolizumab in advanced solid tumor patients naïve or experienced for immune checkpoint blockade
Abstract
Background: This phase 1b study (NCT02323191) evaluated the safety, antitumor activity, pharmacokinetics, and pharmacodynamics of colony-stimulating factor-1 receptor-blocking monoclonal antibody (mAb) emactuzumab in combination with the programmed cell death-1 ligand (PD-L1)-blocking mAb atezolizumab in patients with advanced solid tumors naïve or experienced for immune checkpoint blockers (ICBs).
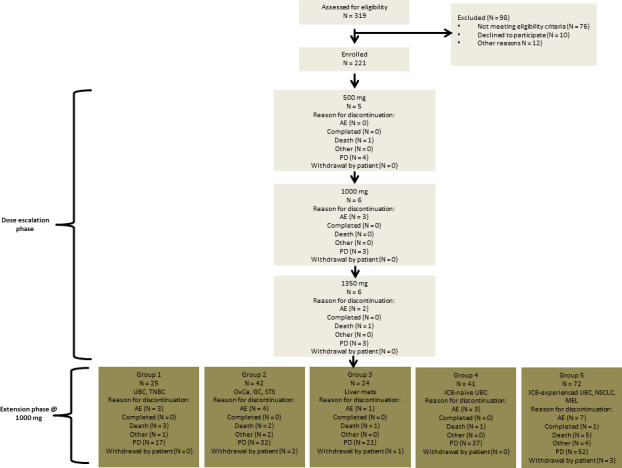
Methods: Emactuzumab (500-1350 mg flat) and atezolizumab (1200 mg flat) were administered intravenously every 3 weeks. Dose escalation of emactuzumab was conducted using the 3+3 design up to the maximum tolerated dose (MTD) or optimal biological dose (OBD). Extension cohorts to evaluate pharmacodynamics and clinical activity were conducted in metastatic ICB-naive urothelial bladder cancer (UBC) and ICB-pretreated melanoma (MEL), non-small cell lung cancer (NSCLC) and UBC patients.
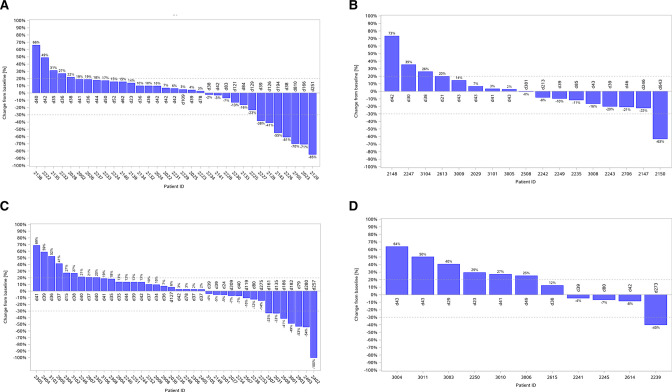
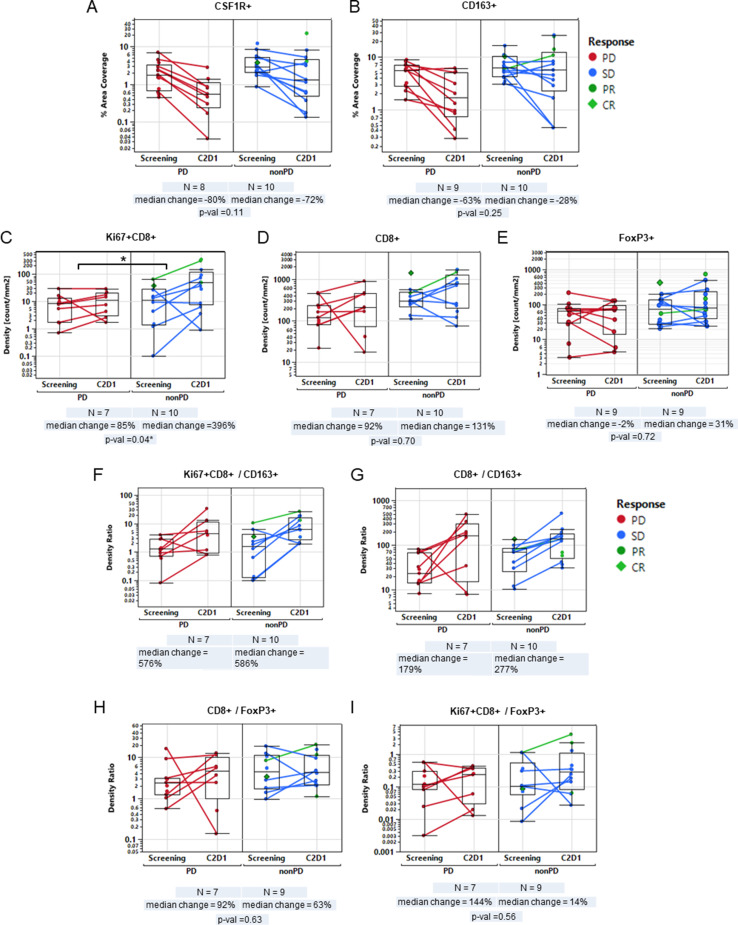
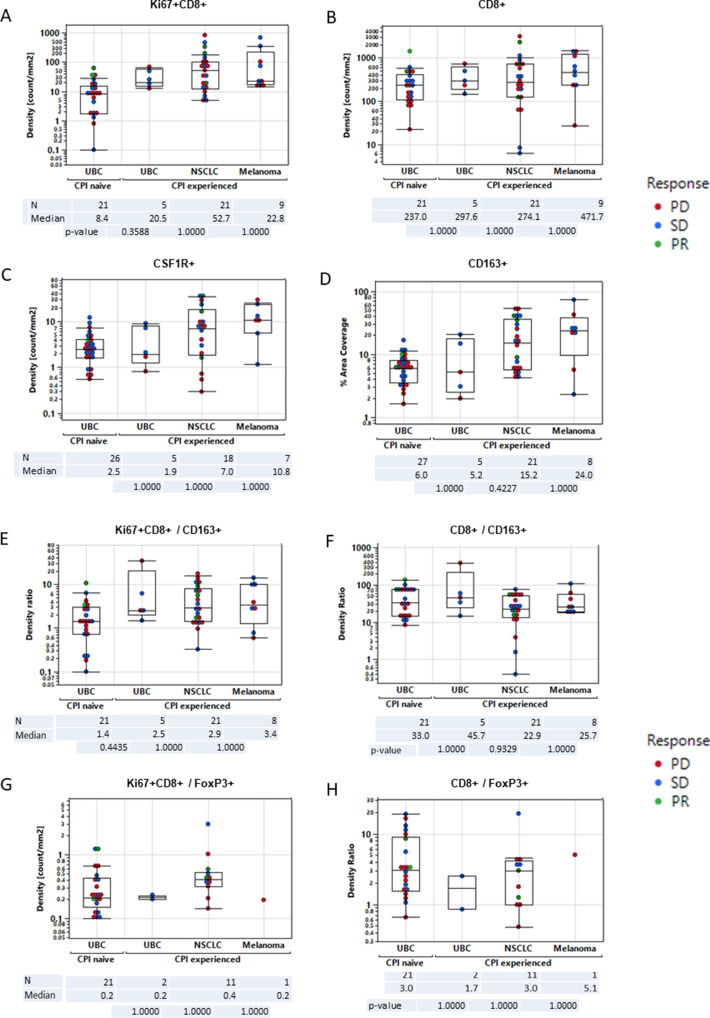
Results: Overall, 221 patients were treated. No MTD was reached and the OBD was determined at 1000 mg of emactuzumab in combination with 1200 mg of atezolizumab. Grade ≥3 treatment-related adverse events occurred in 25 (11.3%) patients of which fatigue and rash were the most common (14 patients (6.3%) each). The confirmed objective response rate (ORR) was 9.8% for ICB-naïve UBC, 12.5% for ICB-experienced NSCLC, 8.3% for ICB-experienced UBC and 5.6% for ICB-experienced MEL patients, respectively. Tumor biopsy analyses demonstrated increased activated CD8 +tumor infiltrating T lymphocytes (TILs) associated with clinical benefit in ICB-naïve UBC patients and less tumor-associated macrophage (TAM) reduction in ICB-experienced compared with ICB-naïve patients.
Conclusion: Emactuzumab in combination with atezolizumab demonstrated a manageable safety profile with increased fatigue and skin rash over usual atezolizumab monotherapy. A considerable ORR was particularly seen in ICB-experienced NSCLC patients. Increase ofCD8 +TILs under therapy appeared to be associated with persistence of a TAM subpopulation.
Keywords: Clinical Trials as Topic; Drug Therapy, Combination; Immunotherapy; Macrophages; T-Lymphocytes.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: CG-R: Invited Speaker: BMS, Eisai, Pierre Fabre, Roche/Genentech; Coordinating PI: BMS; Steering Committee Member: BMS; Local PI: Foundation Medicine; Steering Committee Member: Genentech; Research Grant: Roche/Genentech; AM: Stock ownership Pegascy, Hifibio Therapeutics, Shattuck Labs, Centessa Pharmaceuticals; Honoraria: BMS, AstraZeneca/MedImmune, Oncovir; Consulting and advisory activities: Lytix Biopharma, Eisai, Pierre Fabre, AstraZeneca, Servier, Roche, Redx Pharma, Sotio, Innate Pharma, ImCheck Therapeutics, MSD, OSE Immunotherapeutics, HIFIBIO Therapeutics, MedinCell, Centessa Pharmaceuticals; Speaker’s bureau: BMS; Research funding: BMS, Boehringer Ingelheim, Transgene, MSD; Travel expenses: MSD, AstraZeneca; SC: Honoraria: Amgen, AstraZeneca, BMS, EISAI, Janssen, MSD, Novartis and Roche; Principal Investigator of Clinical Trials for: Amgen, MSD, Sanofi Aventis, Transgene; Advisory Board: Alderaan Biotechnology, Amgen, AstraZeneca, Oncovita, Seagen, Ultrahuman; Travel and congress: AstraZeneca, MSD, Roche; Principal/sub-investigator of clinical trials for: Abbvie, Adaptimmune, Adlai Nortye USA Inc, Aduro Biotech, Agios Pharmaceuticals, Amgen, Argen-X Bvba, Astex Pharmaceuticals, Astra Zeneca Ab, Aveo, Basilea Pharmaceutica International Ltd, Bayer Healthcare Ag, Bbb Technologies Bv, Beigene, BicycleTx Ltd, Blueprint Medicines, Boehringer Ingelheim, Boston Pharmaceuticals, Bristol Myers Squibb, Ca, Celgene Corporation, Chugai Pharmaceutical Co, Clovis Oncology, Cullinan-Apollo, Curevac, Daiichi Sankyo, Debiopharm, Eisai, Eisai Limited, Eli Lilly, Exelixis, Faron Pharmaceuticals Ltd, Forma Tharapeutics, Gamamabs, Genentech, Glaxosmithkline, H3 Biomedicine, Hoffmann La Roche Ag, Imcheck Therapeutics, Innate Pharma, Institut De Recherche Pierre Fabre, Iris Servier, Iteos Belgium SA, Janssen Cilag, Janssen Research Foundation, Kura Oncology, Kyowa Kirin Pharm. Dev, Lilly France, Loxo Oncology, Lytix Biopharma As, Medimmune, Menarini Ricerche, Merck Sharp & Dohme Chibret, Merrimack Pharmaceuticals, Merus, Millennium Pharmaceuticals, Molecular Partners Ag, Nanobiotix, Nektar Therapeutics, Novartis Pharma, Octimet Oncology Nv, Oncoethix, Oncopeptides, Orion Pharma, Ose Pharma, Pfizer, Pharma Mar, Pierre Fabre, Medicament, Roche, Sanofi Aventis, Seattle Genetics, Sotio A.S, Syros Pharmaceuticals, Taiho Pharma, Tesaro, Turning Point Therapeutics, Xencor; Research Grants from: Astrazeneca, BMS, Boehringer Ingelheim, GSK, INCA, Janssen Cilag, Merck, Novartis, Pfizer, Roche, SanofiNon-financial support (drug supplied) from Astrazeneca, Bayer, BMS, Boringher Ingelheim, GSK, Medimmune, Merck, NH TherAGuiX, Pfizer, Roche; SA: Speakers bureau: Pfizer, Roche, Sanofi and BMSAdvisory board: Sanofi; PC: Honoraria: Novartis, Roche/Genentech, Amgen, Astra Zeneca, Merck Serono; Research Funding: Novartis, Roche/Genentech, Lilly, lueprint Medicines, Bayer, Astra Zeneca, Celgene, Plexxikon, Abbvie, BMS, Merck Serono, Merck Sharp and Dohme, Taiho Pharmaceutical, Toray Industries, Transgene, Loxo, GSK, Innate Pharma, Janssen; Travel expenses: Roche, Amgen, Novartis, BMS, MSD, Netris Pharma, Bayer, Merck Serono; DZ: Reports research support from: Roche, Astra Zeneca, and Plexxikon; Personal/consultancy fees from Synlogic Therapeutics, GSK, Roche, Xencor, Memgen, Immunos, Celldex, Calidi, and Agenus; J-PM: Advisory board member or speaker with honoraria: Pfizer, Roche, Astra/Zeneca, Bayer, Innate, Merck Serono, Boerhinger, BMS, Novartis, Janssen, Incyte, Cue Biopharma, ALX Oncology, iTEOS, eTheRNATravel expenses: Amgen, BMS, Pfizer, MSDData safety monitoring board with honoraria: Debio, Nanobiotix, Psioxus; Uncompensated advisory role: MSD; JLPG; Research grants and support: Roche, BMS, MSD, Seattle Genetics. Speakers bureau and advisory boards: Roche, BMS, Ipsen, MSD, Seattle Genetics. Travel support: Roche, MSD, BMS; FSH: Consulting: BMS, Merck, EMD Serono, Novartis, Sanofi, Psioxus Therapeutics, Pieris Pharmacutical, Corner Therapeutics, Eisai, Idera, Takeda, Genentech/Roche; Advisory Board: Compass Therapeutics, Apricity Scientific, Pionyr, Torque, Rheos, Bicara, Checkpoint Therapeutics, Bioentre, Gossamer, Iovance; ATG: Personal fees from: Boehringer-Ingelheim, BMS, MSD, Roche, Pfizer, Astra Zeneca, Tesaro-GSK and non-financial support from Boehringer-Ingelheim, Lilly and RocheMaria Martinez Garcia; Research grants and support: Roche, BMS, MSD, Seattle Genetics; Speakers bureau and advisory boards: Roche, BMS, Ipsen, MSD, Seattle Genetics; Travel support: Roche, MSD, BMS; VB: Consulting or Advisory Role: Puma Biotechnology; Ideaya Biosciences; Loxo Therapeutics, CytomX Therapeutics; Guidepoint; Oncoart; Amunix; Institutional financial support for clinical trials from: Abbvie, ACEO, Adaptaimmune, Amcure, AMGEN, AstraZeneca, BMS, Cytomx, GSK, Genentech/Roche, H3, Incyte, Janssen, Kura, Lilly, Loxo, Nektar, Macrogenics, Menarini, Merck, Merus, Nanobiotix, Novartis, Pfizer, PharmaMar, Principia, PUMA, Sanofi, Taiho, Tesaro, BeiGene, Transgene, Takeda, Incyte, Innovio, MSD, PsiOxus, Seattle Genetics, Mersana, GSK, Daiichi, Nektar, Astellas, ORCA, Boston Therapeutics, Dynavax, DebioPharm, Boehringen Ingelheim, Regeneron, Millenium, Synthon, Spectrum, Rigontec, Zenith; JPE: The author declares no potential conflicts of interest. NH: The author declares no potential conflicts of interest. RS: Consultant/advisory boards: Asana Biosciences, AstraZeneca, Bristol-Myers Squibb, Eisai, Iovance, Merck, Novartis, OncoSec, Pfizer, Replimune; Research funding: Amgen, Merck; DM: Consulting and honoraria: BMS, Pfizer, Merck, Alkermes Inc., EMD Serono, Eli Lilly and Company, Iovance, Eisai Inc., Werewolf Therapeutics, Calithera Biosciences; Research support: BMS, Merck, Genentech, Pfizer, Exelixis, X4 Pharma, Alkermes Inc; MAC: Sponsor employee and sponsor stock ownership; A-MJ: Former sponsor employee and has patent issued in the use of emactuzumab; WJ: Sponsor employee and sponsor stock ownership; CR: Former Roche employee and has patent issued in the use of emactuzumab. Consultant for Verseau Therapeutics, Ridgeline Discovery, iOmx Therapeutics AG; KK: Sponsor employee and Roche stocks; GB: Sponsor employee; FM: Sponsor employee; RC: Sponsor employee and Roche stocks; CW: Sponsor consultantGeorgina Meneses-LorenteSponsor employee; MW: Sponsor employee, stock options, and has patent issued in the use of emactuzumab; DR: Sponsor employee, sponsor stock ownership and has patent issued in the use of emactuzumab; J-PD: Consulting/Advisory: Novartis, Roche/Genentech, BMS, MSD; Research funding: Genentech, BMS, MSD, Astra Zeneca, Transgene; CT: Research funding GSK, travel expenses Mundipharma.
Figures
References
-
- West HJ. JAMA oncology patient page. Immune Checkpoint Inhibitors. JAMA Oncol 2015;1:115. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials