

Suboptimal HIV suppression is associated with progression of coronary artery stenosis: The Multicenter AIDS Cohort Study (MACS) longitudinal coronary CT angiography study
- PMID: 35577614
- PMCID: PMC9950757
- DOI: 10.1016/j.atherosclerosis.2022.04.019
Suboptimal HIV suppression is associated with progression of coronary artery stenosis: The Multicenter AIDS Cohort Study (MACS) longitudinal coronary CT angiography study
Abstract
Background and aims: People living with HIV (HIV+) are surviving longer due to effective antiretroviral therapy. Cardiovascular disease is a leading cause of non-AIDS related clinical events. We determined HIV-related factors associated with coronary artery stenosis progression.
Methods: We performed serial coronary CT angiography among HIV+ and HIV-uninfected (HIV-) men in the Multicenter AIDS Cohort Study. The median inter-scan interval was 4.5 years. Stenosis was graded as 0, 1-29, 30-49, 50-69 or ≥70%. Progression was defined as an increase ≥2 categories. Suppressed HIV infection was consistent viral loads <50 copies/mL allowing 1 "blip" <500 copies/mL, otherwise considered viremic. Multivariable Poisson regression analysis assessed adjusted associations between HIV serostatus and viremia with coronary stenosis progression.
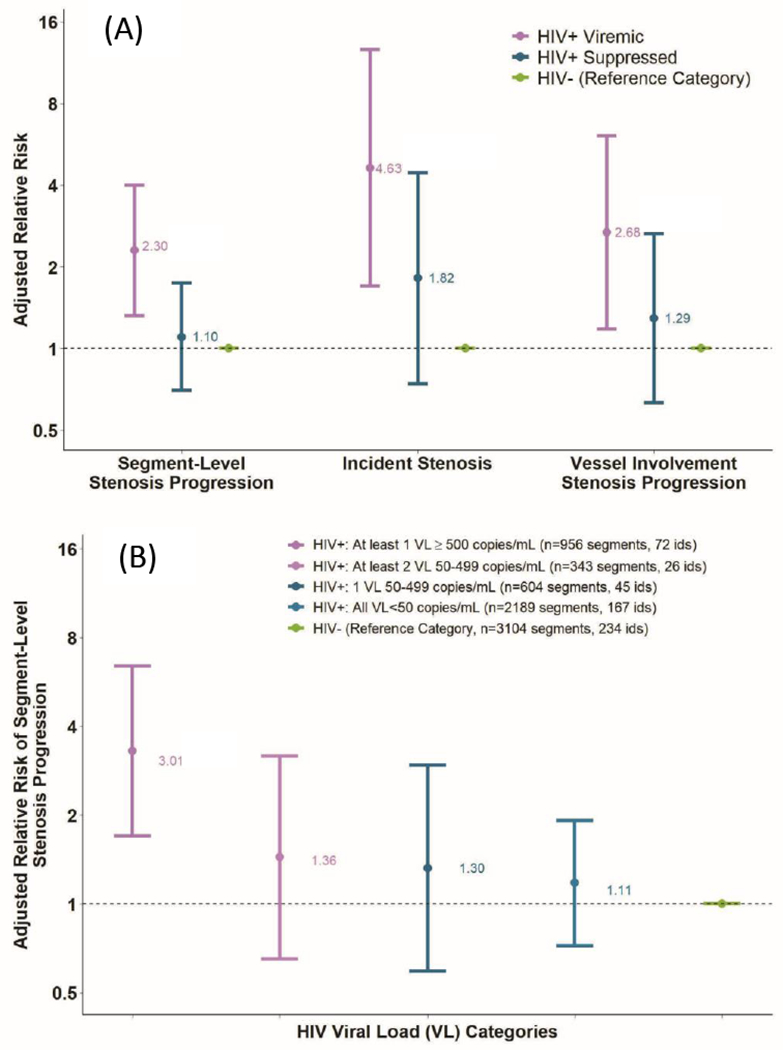
Results: The sample included 310 HIV+ (31% viremic) and 234 HIV- men. The median age was 53 years, 30% Black and 23% current smokers. Viremic men were 2.3 times more likely to develop coronary stenosis progression than HIV- men (adjusted RR 2.30; 95% CI, 1.32-4.00, p = 0.003), with no difference in progression between HIV+ suppressed and HIV- men (RR 1.10; 95% CI, 0.70-1.74, p = 0.67). There was a progressive increase in adjusted relative risk with greater viremia (p = 0.03). Men with >1 viral load >500 copies/ml demonstrated greatest stenosis progression (RR 3.01; 95% CI, 1.53-4.92, p = 0.001 compared with HIV- men). Suppressed HIV+ men with suboptimal antiretroviral adherence had greater stenosis progression (RR 1.91; 95% CI 1.12-3.24, p = 0.02) than HIV + suppressed men with optimal adherence.
Conclusions: Coronary artery stenosis progression was associated with suboptimal HIV RNA suppression and antiretroviral therapy adherence. Effective ongoing HIV virologic suppression and antiretroviral therapy adherence may mitigate risk for coronary disease events among people living with HIV.
Keywords: Atherosclerosis; Coronary CT angiography; Coronary artery disease; Epidemiology; HIV.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of competing interest:
TTB has served as a consultant to Gilead Sciences, ViiV Healthcare, Janssen, Merck, and Theratechnologies. FJP is a consultant and/or on the Speakers’ Bureau for Gilead, Janssen, ViiV and Merck. The remaining authors do not have any relationship with industry.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

Comment in
-
People living with human immunodeficiency virus: Cardiovascular risk screening for an early and effective risk management.Atherosclerosis. 2022 Jul;353:28-29. doi: 10.1016/j.atherosclerosis.2022.06.001. Epub 2022 Jun 8. Atherosclerosis. 2022. PMID: 35710494 No abstract available.
References
-
- Wada N, Jacobson LP, Cohen M, French A, Phair J, Munoz A. Cause-specific life expectancies after 35 years of age for human immunodeficiency syndrome-infected and human immunodeficiency syndrome-negative individuals followed simultaneously in long-term cohort studies, 1984-2008. American journal of epidemiology. 2013;177(2):116–25. - PMC - PubMed
-
- Lerner AM, Eisinger RW, Fauci AS. Comorbidities in Persons With HIV: The Lingering Challenge. JAMA. 2019. - PubMed
-
- Strategies for Management of Antiretroviral Therapy Study G, El-Sadr WM, Lundgren J, Neaton JD, Gordin F, Abrams D, et al. CD4+ count-guided interruption of antiretroviral treatment. The New England journal of medicine. 2006;355(22):2283–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
