

Evaluation of anterior cruciate ligament surgical reconstruction through finite element analysis
- PMID: 35577879
- PMCID: PMC9110399
- DOI: 10.1038/s41598-022-11601-1
Evaluation of anterior cruciate ligament surgical reconstruction through finite element analysis
Abstract
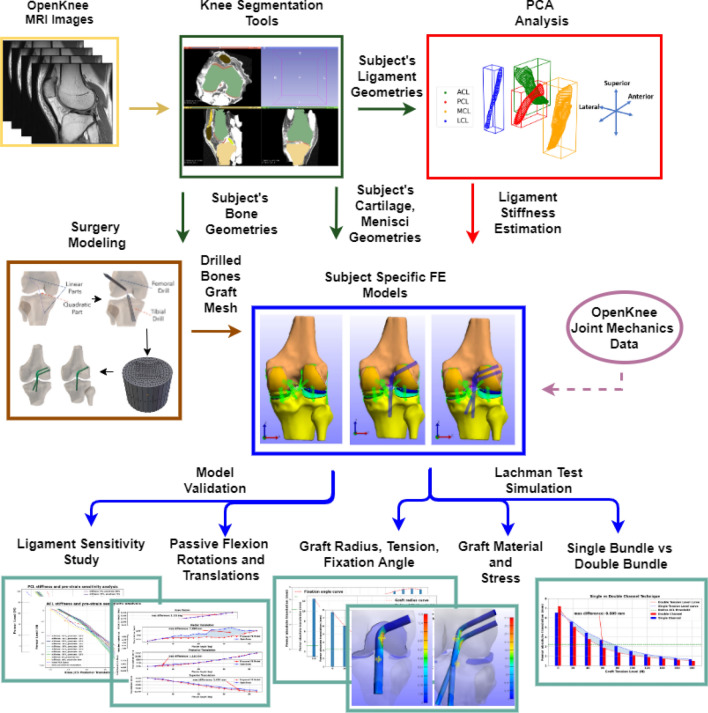
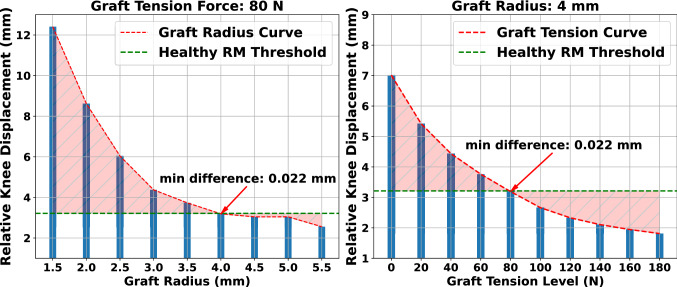
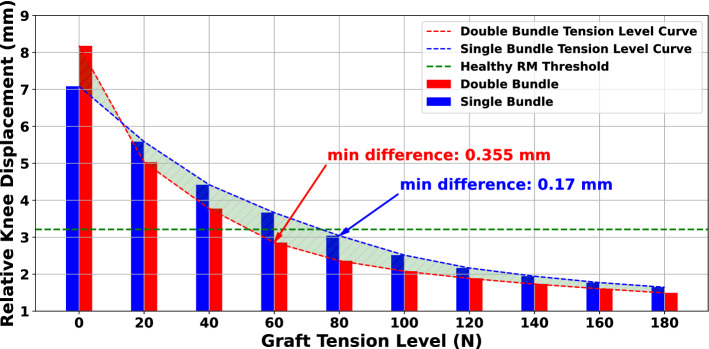
Anterior cruciate ligament (ACL) tear is one of the most common knee injuries. The ACL reconstruction surgery aims to restore healthy knee function by replacing the injured ligament with a graft. Proper selection of the optimal surgery parameters is a complex task. To this end, we developed an automated modeling framework that accepts subject-specific geometries and produces finite element knee models incorporating different surgical techniques. Initially, we developed a reference model of the intact knee, validated with data provided by the Open Knee(s) project. This helped us evaluate the effectiveness of estimating ligament stiffness directly from MRI. Next, we performed a plethora of "what-if" simulations, comparing responses with the reference model. We found that (a) increasing graft pretension and radius reduces relative knee displacement, (b) the correlation of graft radius and tension should not be neglected, (c) graft fixation angle of 20[Formula: see text] can reduce knee laxity, and (d) single-versus double-bundle techniques demonstrate comparable performance in restraining knee translation. In most cases, these findings confirm reported values from comparative clinical studies. The numerical models are made publicly available, allowing for experimental reuse and lowering the barriers for meta-studies. The modeling approach proposed here can complement orthopedic surgeons in their decision-making.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Laskowski, E. Acl injury and rehabilitation. Curr. Phys. Med. Rehabil. Rep.2. 10.1007/s40141-013-0036-8 (2014).
-
- Wetters, N., Weber, A., Wuerz, T., Schub, D. & Mandelbaum, B. Mechanism of injury and risk factors for anterior cruciate ligament injury. Oper. Tech. Sp. Med.24. 10.1053/j.otsm.2015.09.001 (2015).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
