

Manual therapy versus advice to stay active for nonspecific back and/or neck pain: a cost-effectiveness analysis
- PMID: 35578230
- PMCID: PMC9109382
- DOI: 10.1186/s12998-022-00431-7
Manual therapy versus advice to stay active for nonspecific back and/or neck pain: a cost-effectiveness analysis
Abstract
Background: Low back and neck pain are the most common musculoskeletal disorders worldwide, and imply suffering and substantial societal costs, hence effective interventions are crucial. The aim of this study was to evaluate the cost-effectiveness of manual therapy compared with advice to stay active for working age persons with nonspecific back and/or neck pain.
Methods: The two interventions were: a maximum of 6 manual therapy sessions within 6 weeks, including spinal manipulation/mobilization, massage and stretching, performed by a naprapath (index group), respectively information from a physician on the importance to stay active and on how to cope with pain, according to evidence-based advice, at 2 occasions within 3 weeks (control group). A cost-effectiveness analysis with a societal perspective was performed alongside a randomized controlled trial including 409 persons followed for one year, in 2005. The outcomes were health-related Quality of Life (QoL) encoded from the SF-36 and pain intensity. Direct and indirect costs were calculated based on intervention and medication costs and sickness absence data. An incremental cost per health related QoL was calculated, and sensitivity analyses were performed.
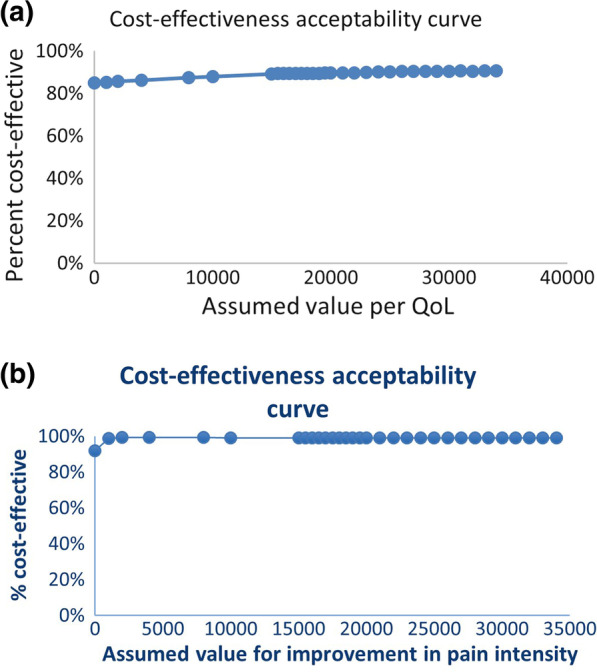
Results: The difference in QoL gains was 0.007 (95% CI - 0.010 to 0.023) and the mean improvement in pain intensity was 0.6 (95% CI 0.068-1.065) in favor of manual therapy after one year. Concerning the QoL outcome, the differences in mean cost per person was estimated at - 437 EUR (95% CI - 1302 to 371) and for the pain outcome the difference was - 635 EUR (95% CI - 1587 to 246) in favor of manual therapy. The results indicate that manual therapy achieves better outcomes at lower costs compared with advice to stay active. The sensitivity analyses were consistent with the main results.
Conclusions: Our results indicate that manual therapy for nonspecific back and/or neck pain is slightly less costly and more beneficial than advice to stay active for this sample of working age persons. Since manual therapy treatment is at least as cost-effective as evidence-based advice from a physician, it may be recommended for neck and low back pain. Further health economic studies that may confirm those findings are warranted. Trial registration Current Controlled Trials ISRCTN56954776. Retrospectively registered 12 September 2006, http://www.isrctn.com/ISRCTN56954776 .
Keywords: Back and neck pain; Cost-effectiveness analysis; Manual therapy; Pain intensity; QoL.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests in connection with the submitted paper.
Figures



References
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
