

Termination-of-resuscitation rule in the emergency department for patients with refractory out-of-hospital cardiac arrest: a nationwide, population-based observational study
- PMID: 35578295
- PMCID: PMC9109290
- DOI: 10.1186/s13054-022-03999-x
Termination-of-resuscitation rule in the emergency department for patients with refractory out-of-hospital cardiac arrest: a nationwide, population-based observational study
Abstract
Background: In Japan, emergency medical service (EMS) providers are prohibited from field termination-of-resuscitation (TOR) in out-of-hospital cardiac arrest (OHCA) patients. In 2013, we developed a TOR rule for emergency department physicians (Goto's TOR rule) immediately after hospital arrival. However, this rule is subject to flaws, and there is a need for revision owing to its relatively low specificity for predicting mortality compared with other TOR rules in the emergency department. Therefore, this study aimed to develop and validate a modified Goto's TOR rule by considering prehospital EMS cardiopulmonary resuscitation (CPR) duration.
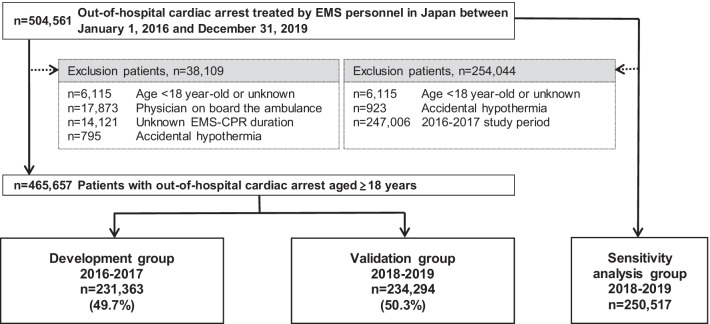
Methods: We analysed the records of 465,657 adult patients with OHCA from the All-Japan Utstein registry from 2016 to 2019 and divided them into two groups: development (n = 231,363) and validation (n = 234,294). The primary outcome measures were specificity, false-positive rate (FPR), and positive predictive value (PPV) of the revised TOR rule in the emergency department for predicting 1-month mortality.
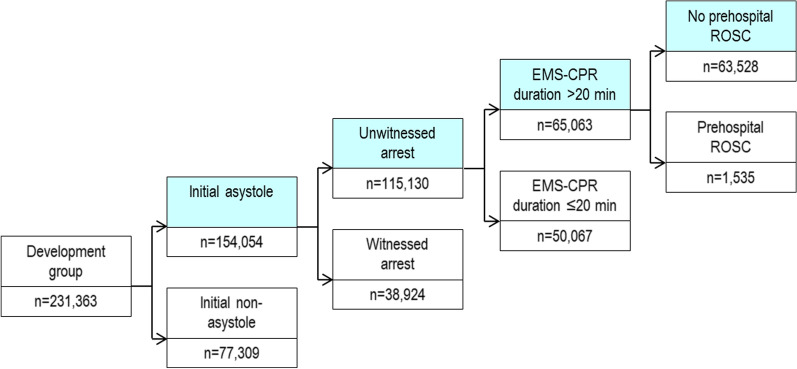
Results: Recursive partitioning analysis for the development group in predicting 1-month mortality revealed that a modified Goto's TOR rule could be defined if patients with OHCA met the following four criteria: (1) initial asystole, (2) unwitnessed arrest by any laypersons, (3) EMS-CPR duration > 20 min, and (4) no prehospital return of spontaneous circulation (ROSC). The specificity, FPR, and PPV of the rule for predicting 1-month mortality were 99.2% (95% confidence interval [CI], 99.0-99.4%), 0.8% (0.6-1.0%), and 99.8% (99.8-99.9%), respectively. The proportion of patients who fulfilled the rule and the area under the receiver operating curve (AUC) was 27.5% (95% CI 27.3-27.7%) and 0.904 (0.902-0.905), respectively. In the validation group, the specificity, FPR, PPV, proportion of patients who met the rule, and AUC were 99.1% (95% CI 98.9-99.2%), 0.9% (0.8-1.1%), 99.8% (99.8-99.8%), 27.8% (27.6-28.0%), and 0.889 (0.887-0.891), respectively.
Conclusion: The modified Goto's TOR rule (which includes the following four criteria: initial asystole, unwitnessed arrest, EMS-CPR duration > 20 min, and no prehospital ROSC) with a > 99% predictor of 1-month mortality is a reliable tool for physicians treating refractory OHCAs immediately after hospital arrival.
Keywords: Cardiopulmonary resuscitation; Emergency department; Epidemiology; Out-of-hospital cardiac arrest; Outcome; Termination-of-resuscitation rule.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Mancini ME, Soar J, Bhanji F, Billi JE, Dennett J, Finn J, et al. Part 12: education, implementation, and teams. 2010 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122:S539–81. - PubMed
-
- Soar J, Mancini ME, Bhanji F, Billi JE, Dennett J, Finn J, et al. Part 12: education, implementation, and teams: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2010;81:e288–330. doi: 10.1016/j.resuscitation.2010.08.030. - DOI - PMC - PubMed
-
- Skrifvars MB, Vayrynen T, Kuisma M, Castren M, Parr MJ, Silfverstople J, et al. Comparison of Helsinki and European Resuscitation Council “do not attempt to resuscitate” guidelines, and a termination of resuscitation clinical prediction rule for out-of-hospital cardiac arrest patients found in asystole or pulseless electrical activity. Resuscitation. 2010;17:679–684. doi: 10.1016/j.resuscitation.2010.01.033. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
