

Accurate and timely diagnosis of Eosinophilic Esophagitis improves over time in Europe. An analysis of the EoE CONNECT Registry
- PMID: 35578565
- PMCID: PMC9189464
- DOI: 10.1002/ueg2.12240
Accurate and timely diagnosis of Eosinophilic Esophagitis improves over time in Europe. An analysis of the EoE CONNECT Registry
Abstract
Background: Poor adherence to clinical practice guidelines for eosinophilic esophagitis (EoE) has been described and the diagnostic delay of the disease continues to be unacceptable in many settings.
Objective: To analyze the impact of improved knowledge provided by the successive international clinical practice guidelines on reducing diagnostic delay and improving the diagnostic process for European patients with EoE.
Methods: Cross-sectional analysis of the EoE CONNECT registry based on clinical practice. Time periods defined by the publication dates of four major sets of guidelines over 10 years were considered. Patients were grouped per time period according to date of symptom onset.
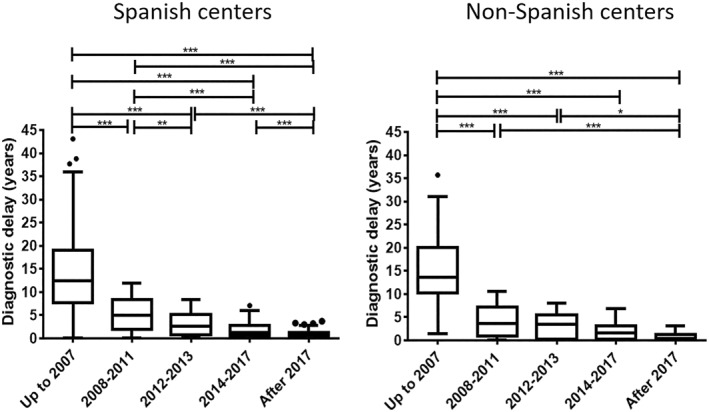
Results: Data from 1,132 patients was analyzed and median (IQR) diagnostic delay in the whole series was 2.1 (0.7-6.2) years. This gradually decreased over time with subsequent release of new guidelines (p < 0.001), from 12.7 years up to 2007 to 0.7 years after 2017. The proportion of patients with stricturing of mixed phenotypes at the point of EoE diagnosis also decreased over time (41.3% vs. 16%; p < 0.001), as did EREFS scores. The fibrotic sub-score decreased from a median (IQR) of 2 (1-2) to 0 (0-1) when patients whose symptoms started up to 2007 and after 2017 were compared (p < 0.001). In parallel, symptoms measured with the Dysphagia Symptoms Score reduced significantly when patients with symptoms starting before 2007 and after 2012 were compared. A reduction in the number of endoscopies patients underwent before the one that achieved an EoE diagnosis, and the use of allergy testing as part of the diagnostic workout of EoE, also reduced significantly over time (p = 0.010 and p < 0.001, respectively).
Conclusion: The diagnostic work-up of EoE patients improved substantially over time at the European sites contributing to EoE CONNECT, with a dramatic reduction in diagnostic delay.
Keywords: Diagnostic delay; Endoscopy; Eosinophilic esophagitis; Gastrointestinal; Guideline Adherence; Practice Guidelines as Topic; Registries.
© 2022 The Authors. United European Gastroenterology Journal published by Wiley Periodicals LLC on behalf of United European Gastroenterology.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures



Comment in
-
Modifying the natural history of gastrointestinal diseases in Europe as a result of early diagnosis: From eosinophilic esophagitis to inflammatory bowel disease.United European Gastroenterol J. 2022 Sep;10(7):612-613. doi: 10.1002/ueg2.12256. Epub 2022 May 25. United European Gastroenterol J. 2022. PMID: 35614522 Free PMC article. No abstract available.
References
-
- Lucendo AJ, Molina‐Infante J, Arias A, Arnim U, Bredenoord AJ, Bussmann C, et al. Guidelines on eosinophilic esophagitis: evidence‐based statements and recommendations for diagnosis and management in children and adults. United Eur Gastroenterol J. 2017;5(3):335–58. 10.1177/2050640616689525 - DOI - PMC - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
