

A Novel Inflammation-Related Gene Signature for Overall Survival Prediction and Comprehensive Analysis in Pediatric Patients with Wilms Tumor
- PMID: 35578692
- PMCID: PMC9107364
- DOI: 10.1155/2022/2651105
A Novel Inflammation-Related Gene Signature for Overall Survival Prediction and Comprehensive Analysis in Pediatric Patients with Wilms Tumor
Abstract
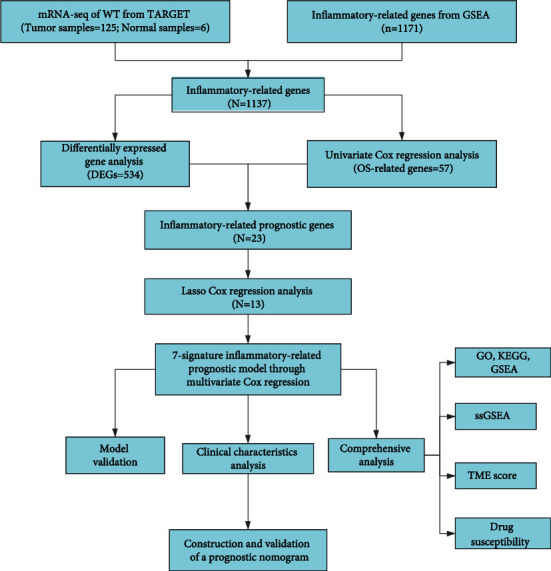
Wilms tumor (WT) is a common pediatric renal cancer, with a poor prognosis and high-risk recurrence in some patients. The inflammatory microenvironment is gradually gaining attention in WT. In this study, novel inflammation-related signatures and prognostic model were explored and integrated using bioinformatics analysis. The mRNA profile of pediatric patients with WT and inflammation-related genes (IRGs) were acquired from Therapeutically Available Research to Generate Effective Treatments (TARGET) and Gene Set Enrichment Analysis (GSEA) databases, respectively. Then, a novel prognostic model founded on 7-IRGs signature (BICC1, CSPP1, KRT8, MYCN, NELFA, NXN, and RNF113A) was established by the least absolute shrinkage and selection operator (LASSO) and multivariate Cox regression to stratify pediatric patients with WT into high- and low-risk groups successfully. And a stable performance of the prognostic risk model was verified in predicting overall survival (OS) by receiver-operating characteristic (ROC) curves, Kaplan-Meier (KM) curves, and independent prognostic analysis (p < 0.05). In addition, a novel nomogram integrating risk scores with good robustness was developed and validated by C-index, ROC, and calibration plots. The potential function and pathway were explored via Gene Ontology (GO), Kyoto Encyclopedia of Genes and Genomes (KEGG), and GSEA, with mainly inflammation and immune-related biological processes. The higher-risk scores, the lower immune infiltration, as shown in the single-sample GSEA (ssGSEA) and tumor microenvironment (TME) analysis. The drug sensitivity analysis showed that regulating 7-IRGs signature has a significant correlation with the chemotherapy drugs of WT patients. In summary, this study defined a prognostic risk model and nomogram based on 7-IRGs signature, which may provide novel insights into clinical prognosis and inflammatory study in WT patients. Besides, enhancing immune infiltration based on inflammatory response and regulating 7-IRGs signature are beneficial to ameliorating the efficacy in WT patients.
Copyright © 2022 Jiahao Zhang et al.
Conflict of interest statement
All authors declare that they have no conflict of interest with the state.
Figures








Similar articles
-
Development and Validation of an Inflammatory Response-Related Gene Signature for Predicting the Prognosis of Pancreatic Adenocarcinoma.Inflammation. 2022 Aug;45(4):1732-1751. doi: 10.1007/s10753-022-01657-6. Epub 2022 Mar 23. Inflammation. 2022. PMID: 35322324
-
Identification of prognostic immune-related gene signature associated with tumor microenvironment of colorectal cancer.BMC Cancer. 2021 Aug 8;21(1):905. doi: 10.1186/s12885-021-08629-3. BMC Cancer. 2021. PMID: 34364366 Free PMC article.
-
Immune Landscape of Gastric Carcinoma Tumor Microenvironment Identifies a Peritoneal Relapse Relevant Immune Signature.Front Immunol. 2021 May 13;12:651033. doi: 10.3389/fimmu.2021.651033. eCollection 2021. Front Immunol. 2021. PMID: 34054812 Free PMC article.
-
Identification of a glycolysis- and lactate-related gene signature for predicting prognosis, immune microenvironment, and drug candidates in colon adenocarcinoma.Front Cell Dev Biol. 2022 Aug 23;10:971992. doi: 10.3389/fcell.2022.971992. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36081904 Free PMC article.
-
The Inflammatory Microenvironment in Wilms Tumors.In: van den Heuvel-Eibrink MM, editor. Wilms Tumor [Internet]. Brisbane (AU): Codon Publications; 2016 Mar. Chapter 12. In: van den Heuvel-Eibrink MM, editor. Wilms Tumor [Internet]. Brisbane (AU): Codon Publications; 2016 Mar. Chapter 12. PMID: 27512766 Free Books & Documents. Review.
Cited by
-
Wilms' Tumor: A Review of Clinical Characteristics, Treatment Advances, and Research Opportunities.Medicina (Kaunas). 2025 Mar 12;61(3):491. doi: 10.3390/medicina61030491. Medicina (Kaunas). 2025. PMID: 40142302 Free PMC article. Review.
-
A novel molecular subtypes and risk model based on inflammatory response-related lncrnas for bladder cancer.Hereditas. 2022 Aug 13;159(1):32. doi: 10.1186/s41065-022-00245-w. Hereditas. 2022. PMID: 35964079 Free PMC article.
-
Exploring the causal relationship between hemoglobin and pancreatic cancer and its potential mechanisms through bioinformatics and Mendelian randomization.Discov Oncol. 2025 Aug 5;16(1):1472. doi: 10.1007/s12672-025-03352-y. Discov Oncol. 2025. PMID: 40762741 Free PMC article.
-
The pan-immune-inflammation value predicts prognosis and chemotherapy-related adverse events in Wilms' tumor patients.BMC Cancer. 2025 Jun 1;25(1):979. doi: 10.1186/s12885-025-14391-7. BMC Cancer. 2025. PMID: 40452012 Free PMC article.
-
Lymph node metastasis related gene BICC1 promotes tumor progression by promoting EMT and immune infiltration in pancreatic cancer.BMC Med Genomics. 2023 Oct 25;16(1):263. doi: 10.1186/s12920-023-01696-4. BMC Med Genomics. 2023. PMID: 37880742 Free PMC article.
References
-
- Daw N. C., Chi Y. Y., Kalapurakal J. A., et al. Activity of vincristine and irinotecan in diffuse anaplastic Wilms tumor and therapy outcomes of stage II to IV disease: results of the children's oncology group AREN0321 study. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology . 2020;38(14):1558–1568. doi: 10.1200/jco.19.01265. - DOI - PMC - PubMed
-
- Howlader N., Noone A. M., Krapcho M., et al. SEER Cancer Statistics Review, 1975-2018. In: Mariotto A., Lewis D. R., Chen H. S., Feuer E. J., Cronin K. A., editors. National Cancer Institute . Bethesda, MD: 2021. October 2021 https://seer.cancer.gov/csr/1975_2018/
-
- Dome J. S., Graf N., Geller J. I., et al. Advances in Wilms tumor treatment and biology: progress through international collaboration. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology . 2015;33(27):2999–3007. doi: 10.1200/JCO.2015.62.1888. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
