

Retrospective, Landmark Analysis of Long-term Adult Morbidity Following Allogeneic HSCT for Inborn Errors of Immunity in Infancy and Childhood
- PMID: 35579633
- PMCID: PMC9537214
- DOI: 10.1007/s10875-022-01278-6
Retrospective, Landmark Analysis of Long-term Adult Morbidity Following Allogeneic HSCT for Inborn Errors of Immunity in Infancy and Childhood
Abstract
Purpose: Allogeneic hematopoietic stem cell transplant (HSCT) remains the treatment of choice for patients with inborn errors of immunity (IEI). There is little published medical outcome data assessing late medical complications following transition to adult care. We sought to document event-free survival (EFS) in transplanted IEI patients reaching adulthood and describe common late-onset medical complications and factors influencing EFS.
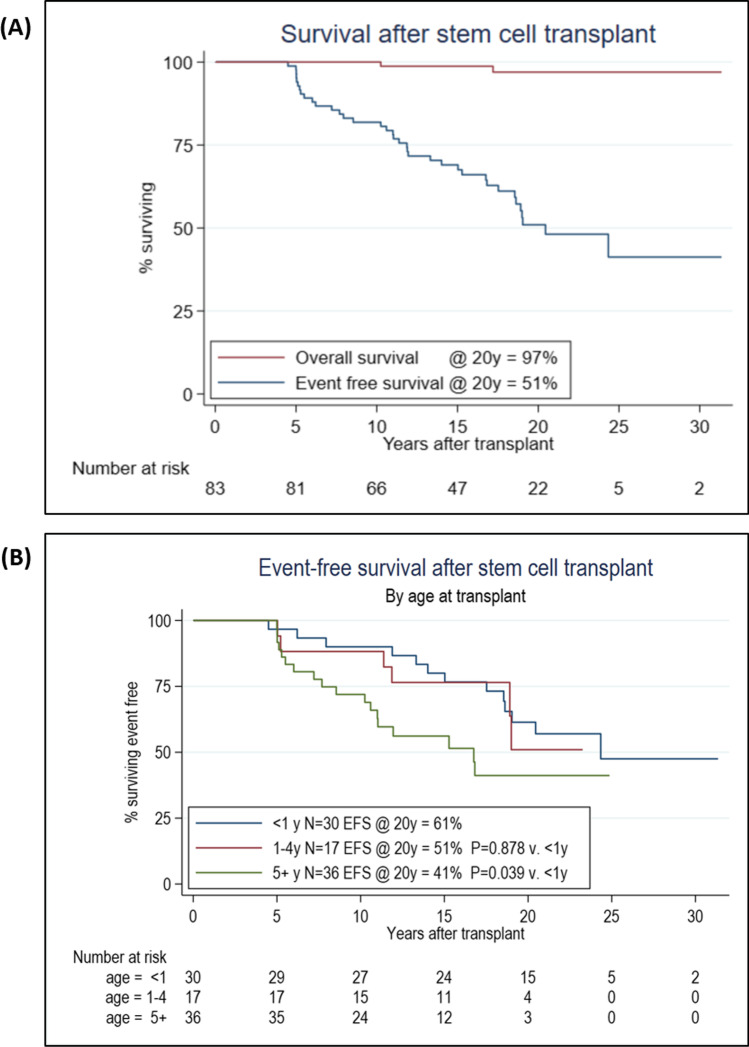
Methods: In this landmark analysis, 83 adults surviving 5 years or more following prior HSCT in childhood for IEI were recruited. The primary endpoint was event-free survival, defined as time post-first HSCT to graft failure, graft rejection, chronic infection, life-threatening or recurrent infections, malignancy, significant autoimmune disease, moderate to severe GVHD or major organ dysfunction. All events occurring less than 5 years post-HSCT were excluded.
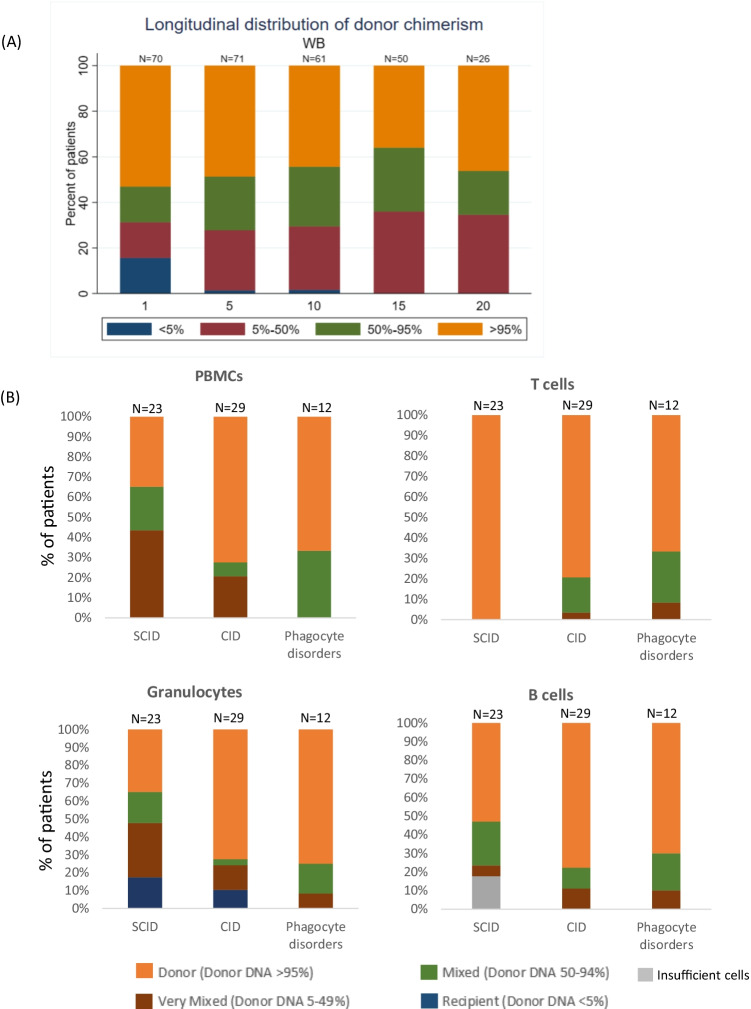
Results: EFS was 51% for the whole cohort at a median of 20 years post HSCT. Multivariable analysis identified age at transplant and whole blood chimerism as independent predictors of long-term EFS. Year of HSCT, donor, conditioning intensity and underlying diagnosis had no significant impact on EFS. 59 events occurring beyond 5 years post-HSCT were documented in 37 patients (45% cohort). A total of 25 patients (30% cohort) experienced ongoing significant complications requiring active medical intervention at last follow-up.
Conclusion: Although most patients achieved excellent, durable immune reconstitution with infrequent transplant-related complications, very late complications are common and associated with mixed chimerism post-HSCT. Early intervention to correct mixed chimerism may improve long-term outcomes and adult health following HSCT for IEI in childhood.
Keywords: Very long-term outcome; allogeneic HSCT for IEI.
© 2022. The Author(s).
Conflict of interest statement
None declared.
Figures
References
-
- Chiesa R, Wang J, Blok HJ, Hazelaar S, Neven B, Moshous D, et al. Haematopoietic Cell Transplantation in Chronic Granulomatous Disease: a Study on 712 Children and Adults. Blood. 2020. - PubMed
-
- Moratto D, Giliani S, Bonfim C, Mazzolari E, Fischer A, Ochs HD, et al. Long-term outcome and lineage-specific chimerism in 194 patients with Wiskott-Aldrich syndrome treated by hematopoietic cell transplantation in the period 1980–2009: an international collaborative study. Blood. 2011;118(6):1675–1684. doi: 10.1182/blood-2010-11-319376. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
