

Totally extraperitoneal laparoscopic inguinal hernia repair post-radical prostatectomy
- PMID: 35579700
- PMCID: PMC9613734
- DOI: 10.1007/s00464-022-09281-z
Totally extraperitoneal laparoscopic inguinal hernia repair post-radical prostatectomy
Abstract
Background: Previous radical prostatectomy (RP) is considered a relative contraindication to the laparoscopic approach for inguinal hernia repair (LIHR). This study aimed to compare feasibility, safety and outcomes for patients undergoing totally extraperitoneal (TEP) LIHR who have previously undergone RP.
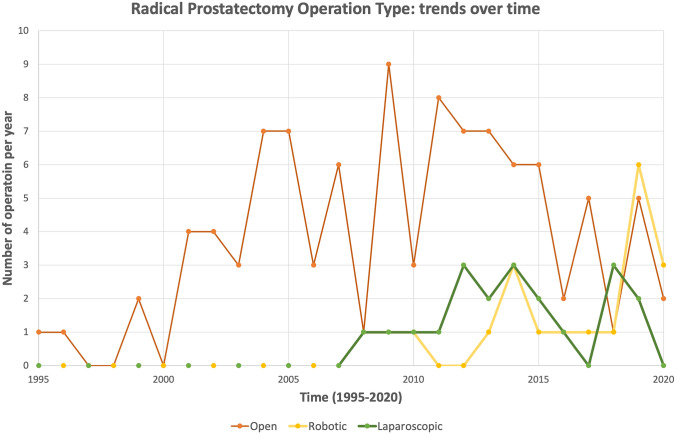
Methods: This single surgeon, case-control study was performed using a prospective database of all patients undergoing TEP LIHR between 1995 and 2020. Patients who underwent previous RP were identified and compared to matched controls. Pre-operative, operative and post-operative data were analysed. The type of RP, open, laparoscopic or robotic, was identified and operative outcomes compared between the three groups.
Results: 6532 LIHR cases were identified. 165 had previously undergone RP and 6367 had undergone primary LIHR without prior RP. The groups were matched for age, demographics and co-morbidities. All operations were commenced laparoscopically, three converted to open in the LIHR + RP group and none in the LIHR group. Median operative time in patients with previous RP was longer, for unilateral (40 min vs. 21 min, p < 0.0001) and bilateral (71 vs. 30 min, p < 0.0001) LIHR. The majority of cases were performed as day stay procedures. There was no difference in immediate recovery parameters including time to discharge, complication rates, return to normal function, return to driving or post-operative analgesia. At 3 months of follow-up there was no difference in hernia recurrence for unilateral (2/128 vs 6/2234, p = 0.0658) or bilateral (0/24 vs 3/1490, p ≥ 0.999) LIHR, nor chronic pain as measured by patient awareness or restriction of activity. No differences in operative and post-operative outcomes were identified between the three types of RP, other than difference in operative time (p = 0.0336).
Conclusions: Previous RP should not be an absolute contraindication for TEP LIHR. Although previous RP adds complexity, in experienced hands TEP LIHR can be done safely, with outcomes equivalent to patients who have not previously undergone RP.
Keywords: Laparoscopic hernia repair; Laparoscopic inguinal hernia repair; Radical prostatectomy; Totally extraperitoneal trans-abdominal preperitoneal.
© 2022. The Author(s).
Conflict of interest statement
Imogen Watt, Adam Bartlett and John Dunn have no conflicts of interest or financial ties to disclose. Andrew Bowker runs teaching and mentoring seminars for surgeons learning laparoscopic inguinal hernia repair, supported by Medtronic, which covers seminar expenses. He has no conflicts of interest or financial ties to disclose.
Figures


References
-
- Lodding P, Bergdahl C, Nyberg M, Pileblad E, Stranne J, Hugosson J. Inguinal hernia after radical retropubic prostatectomy for prostate cancer: a study of incidence and risk factors in comparison to no operation and lymphadenectomy. J Urol. 2001;166(3):964–967. doi: 10.1016/S0022-5347(05)65874-0. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
