

Circulating free testosterone and risk of aggressive prostate cancer: Prospective and Mendelian randomisation analyses in international consortia
- PMID: 35579976
- PMCID: PMC7613289
- DOI: 10.1002/ijc.34116
Circulating free testosterone and risk of aggressive prostate cancer: Prospective and Mendelian randomisation analyses in international consortia
Abstract
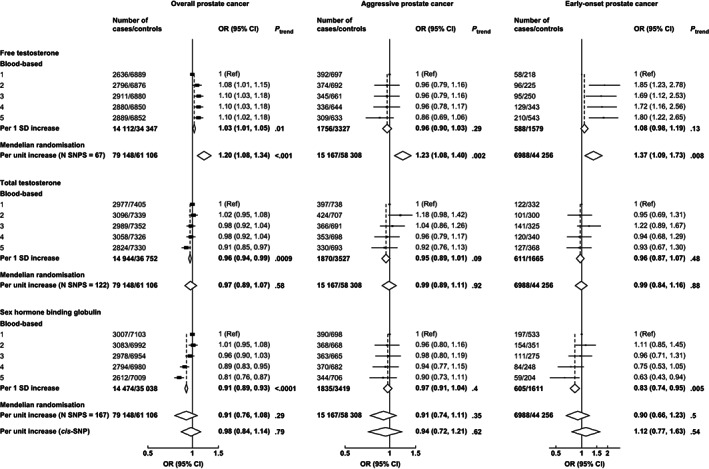
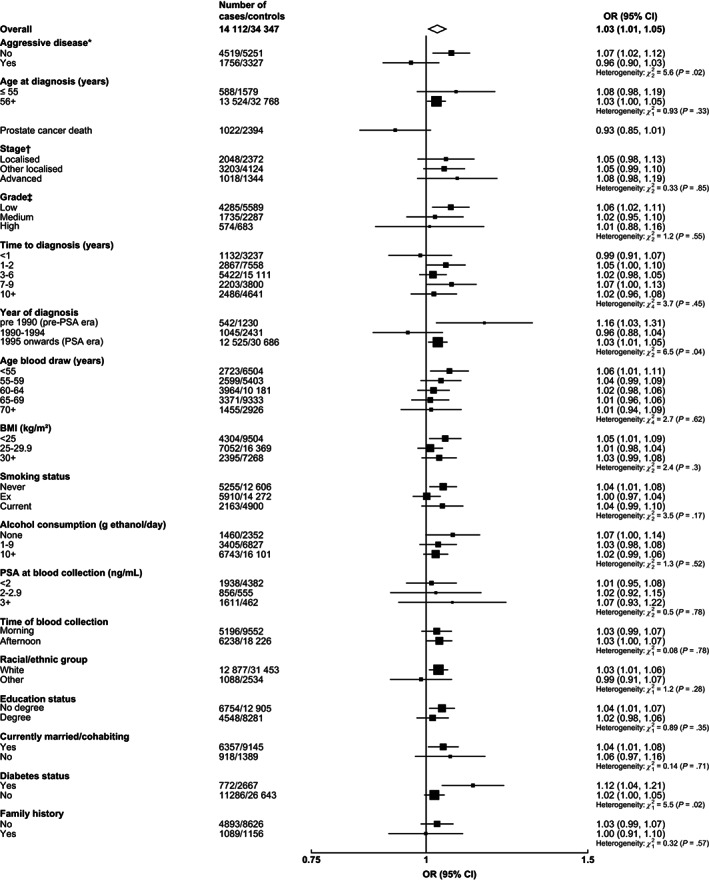
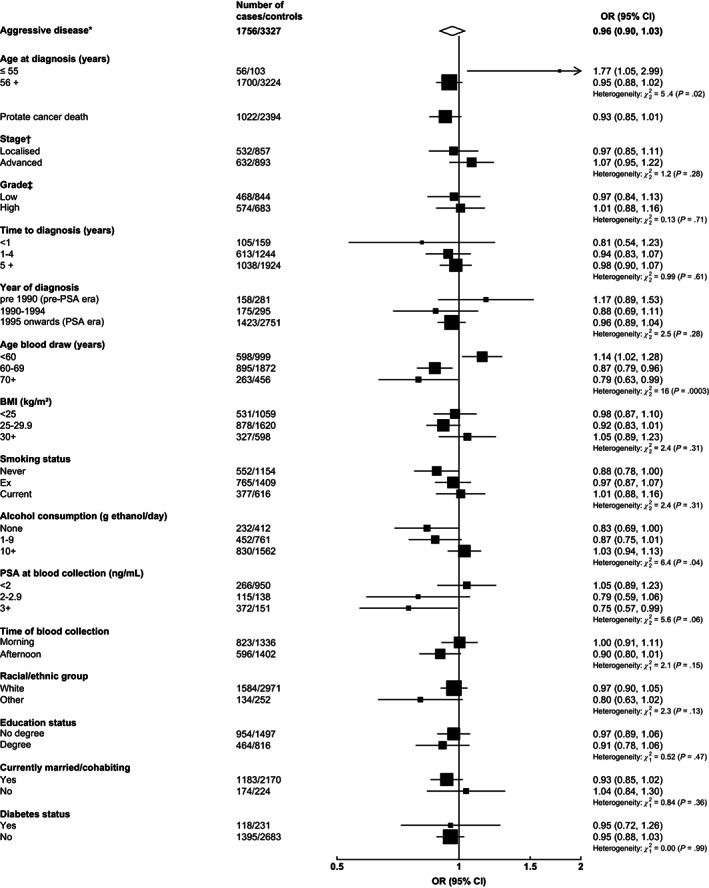
Previous studies had limited power to assess the associations of testosterone with aggressive disease as a primary endpoint. Further, the association of genetically predicted testosterone with aggressive disease is not known. We investigated the associations of calculated free and measured total testosterone and sex hormone-binding globulin (SHBG) with aggressive, overall and early-onset prostate cancer. In blood-based analyses, odds ratios (OR) and 95% confidence intervals (CI) for prostate cancer were estimated using conditional logistic regression from prospective analysis of biomarker concentrations in the Endogenous Hormones, Nutritional Biomarkers and Prostate Cancer Collaborative Group (up to 25 studies, 14 944 cases and 36 752 controls, including 1870 aggressive prostate cancers). In Mendelian randomisation (MR) analyses, using instruments identified using UK Biobank (up to 194 453 men) and outcome data from PRACTICAL (up to 79 148 cases and 61 106 controls, including 15 167 aggressive cancers), ORs were estimated using the inverse-variance weighted method. Free testosterone was associated with aggressive disease in MR analyses (OR per 1 SD = 1.23, 95% CI = 1.08-1.40). In blood-based analyses there was no association with aggressive disease overall, but there was heterogeneity by age at blood collection (OR for men aged <60 years 1.14, CI = 1.02-1.28; Phet = .0003: inverse association for older ages). Associations for free testosterone were positive for overall prostate cancer (MR: 1.20, 1.08-1.34; blood-based: 1.03, 1.01-1.05) and early-onset prostate cancer (MR: 1.37, 1.09-1.73; blood-based: 1.08, 0.98-1.19). SHBG and total testosterone were inversely associated with overall prostate cancer in blood-based analyses, with null associations in MR analysis. Our results support free testosterone, rather than total testosterone, in the development of prostate cancer, including aggressive subgroups.
Keywords: Mendelian randomisation; SHBG; aggressive prostate cancer; prostate cancer; testosterone.
© 2022 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Conflict of interest statement
Dr Michael V. Holmes declares unpaid consultancy for Boehringer Ingelheim. The other authors have no conflicts to disclose.
Figures
References
-
- Ferlay J, Ervik M, Lam F, et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer; 2018.
Publication types
MeSH terms
Substances
Grants and funding
- U01 CA167462/CA/NCI NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- UG1 CA189974/CA/NCI NIH HHS/United States
- U01 CA167552/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U01 CA086308/CA/NCI NIH HHS/United States
- Z99 CA999999/ImNIH/Intramural NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- A29019/CRUK_/Cancer Research UK/United Kingdom
- 29019/CRUK_/Cancer Research UK/United Kingdom
- U01 AG018033/AG/NIA NIH HHS/United States
- A19170/CRUK_/Cancer Research UK/United Kingdom
- 29017/CRUK_/Cancer Research UK/United Kingdom
- U01 CA063673/CA/NCI NIH HHS/United States
- U01 CA182883/CA/NCI NIH HHS/United States
- UM1 CA167462/CA/NCI NIH HHS/United States
- P30 CA071789/CA/NCI NIH HHS/United States
- 001/WHO_/World Health Organization/International
- U01 CA164973/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
