

Mind the gap: Mapping variation between national and local clinical practice guidelines for acute paediatric asthma from the United Kingdom and the Netherlands
- PMID: 35580117
- PMCID: PMC9113591
- DOI: 10.1371/journal.pone.0267445
Mind the gap: Mapping variation between national and local clinical practice guidelines for acute paediatric asthma from the United Kingdom and the Netherlands
Abstract
Background: Clinical practice guidelines (CPGs) aim to standardize clinical care. Increasingly, hospitals rely on locally produced guidelines alongside national guidance. This study examines variation between national and local CPGs, using the example of acute paediatric asthma guidance from the United Kingdom and the Netherlands.
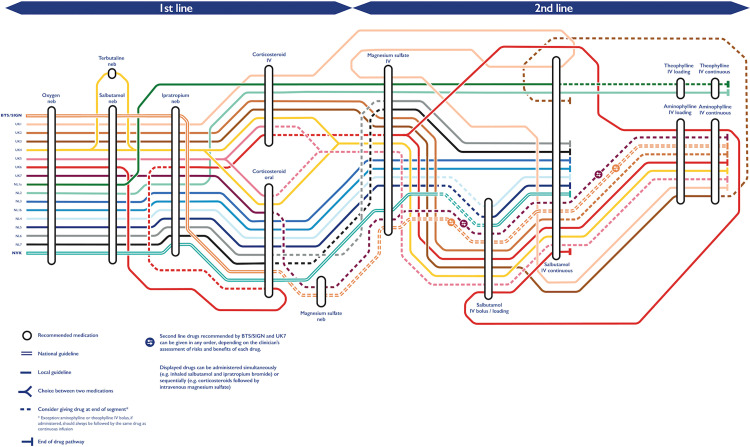
Methods: Fifteen British and Dutch local CPGs were collected with the matching national guidance for the management of acute asthma in children under 18 years old. The drug sequences, routes and methods of administration recommended for patients with severe asthma and the tone of recommendation across both types of CPGs were schematically represented. Deviations from national guidance were measured. Variation in recommended doses of intravenous salbutamol was examined. CPG quality was assessed using the Appraisal of Guidelines for Research and Evaluation (AGREE) II.
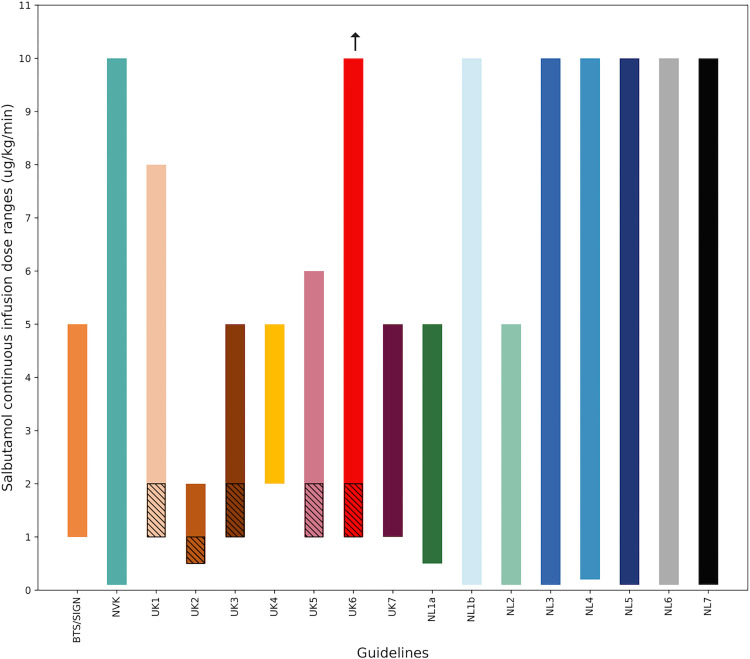
Results: British and Dutch national CPGs differed in the recommended drug choices, sequences, routes and methods of administration for severe asthma. Dutch national guidance was more rigidly defined. Local British CPGs diverged from national guidance for 23% of their recommended interventions compared to 8% for Dutch local CPGs. Five British local guidelines and two Dutch local guidelines differed from national guidance for multiple treatment steps. Variation in second-line recommendations was greater than for first-line recommendations across local CPGs from both countries. Recommended starting doses for salbutamol infusions varied by more than tenfold. The quality of the sampled local CPGs was low across all AGREE II domains.
Conclusions: Local CPGs for the management of severe acute paediatric asthma featured substantial variation and frequently diverged from national guidance. Although limited to one condition, this study suggests that unmeasured variation across local CPGs may contribute to variation of care more broadly, with possible effects on healthcare quality.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: two authors (NA and CK) had support from the National Institute for Health Research and one author (JC) had support from the Wellcome Trust for the submitted work. NA is the CEO of Dosium, a software company building decision support tools for medication safety. Authors had no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Paediatric acute asthma management in Australia and New Zealand: practice patterns in the context of clinical practice guidelines.Arch Dis Child. 2008 Apr;93(4):307-12. doi: 10.1136/adc.2007.125062. Arch Dis Child. 2008. PMID: 18356383
-
Systematic Review and Critical Appraisal of Urticaria Clinical Practice Guidelines: A Global Guidelines in Dermatology Mapping Project (GUIDEMAP).J Allergy Clin Immunol Pract. 2023 Oct;11(10):3213-3220.e11. doi: 10.1016/j.jaip.2023.07.002. Epub 2023 Jul 13. J Allergy Clin Immunol Pract. 2023. PMID: 37451615
-
Appraisal of Australian and New Zealand paediatric sepsis guidelines.Emerg Med Australas. 2024 Jun;36(3):436-442. doi: 10.1111/1742-6723.14381. Epub 2024 Feb 25. Emerg Med Australas. 2024. PMID: 38403429
-
The administration of beta2-agonists for paediatric asthma and its adverse reaction in Australian and New Zealand emergency departments: a cross-sectional survey.Eur J Emerg Med. 2003 Sep;10(3):219-24. doi: 10.1097/00063110-200309000-00012. Eur J Emerg Med. 2003. PMID: 12972899
-
Are paediatric clinical practice guidelines trustworthy?J Paediatr Child Health. 2019 Sep;55(9):1044-1055. doi: 10.1111/jpc.14567. Epub 2019 Jul 27. J Paediatr Child Health. 2019. PMID: 31350939 Review.
References
-
- Institute of Medicine (U.S.). Committee on Standards for Developing Trustworthy Clinical Practice Guidelines. Clinical practice guidelines we can trust [Internet]. Washington DC;2011[cited 2020 Jun 23]. 266 p. Report No: 978-0-309-16422-1. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209539/.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
