

Trading spaces: Medicare's regulatory spillovers on treatment setting for non-Medicare patients
- PMID: 35580506
- PMCID: PMC10371213
- DOI: 10.1016/j.jhealeco.2022.102624
Trading spaces: Medicare's regulatory spillovers on treatment setting for non-Medicare patients
Abstract
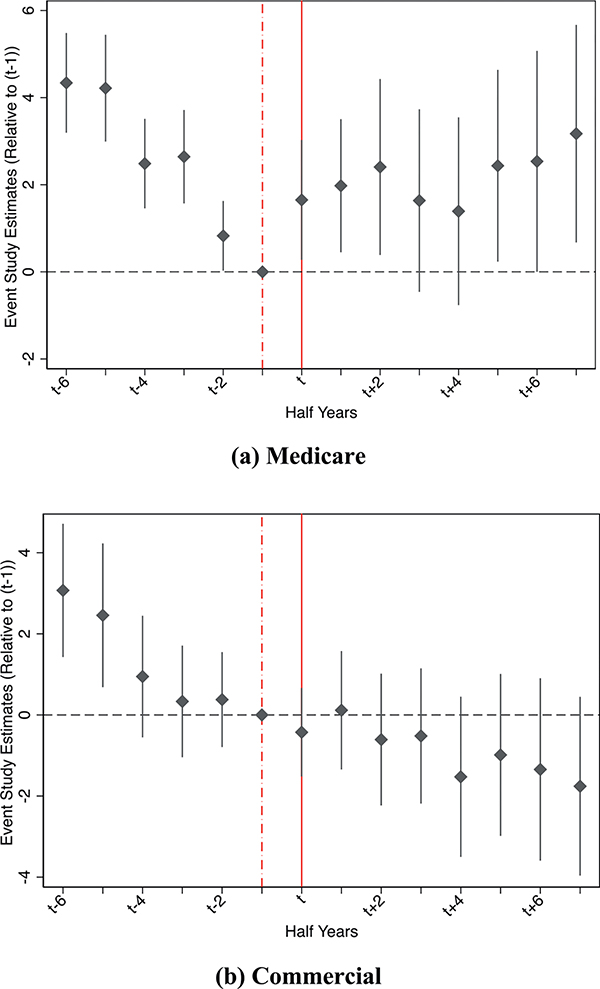
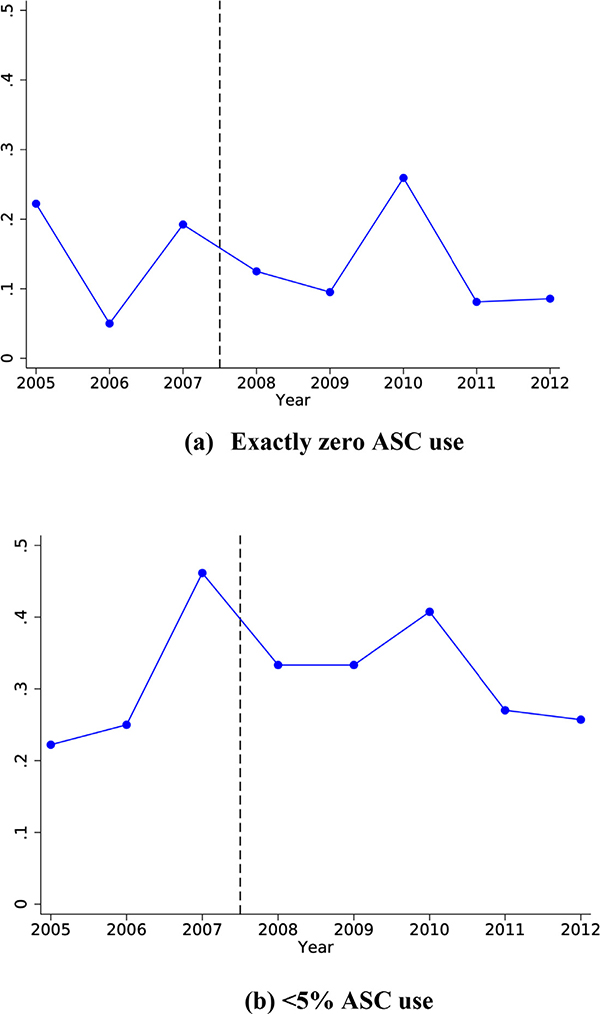
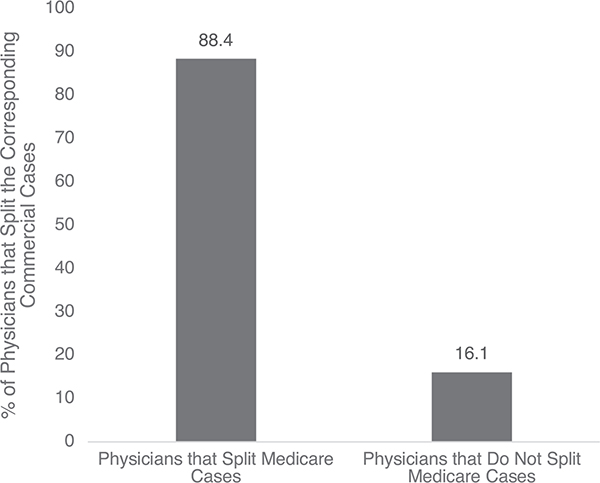
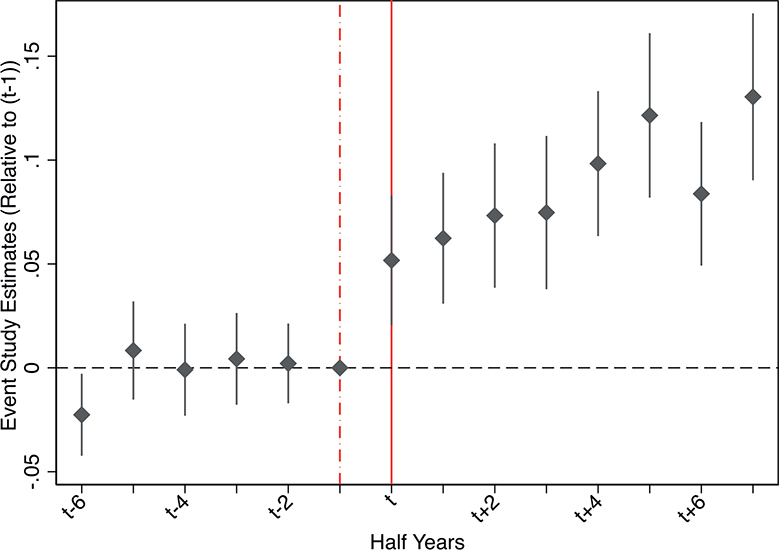
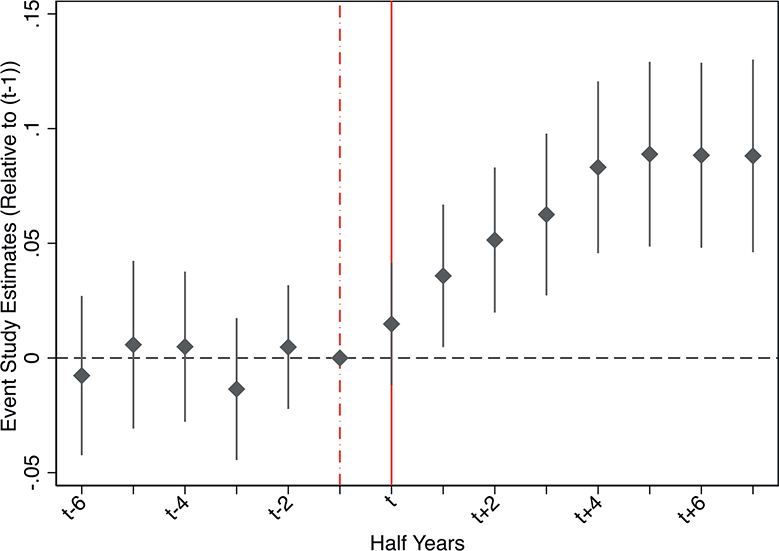
Medicare pricing is known to indirectly influence provider prices and care provision for non-Medicare patients; however, Medicare's regulatory externalities beyond fee-setting are less well understood. We study how physicians' outpatient surgery choices for non-Medicare patients responded to Medicare removing a ban on ambulatory surgery center (ASC) use for a specific procedure. Following the rule change, surgeons began reallocating both Medicare and commercially insured patients to ASCs. Specifically, physicians became 70% more likely to use ASCs for the policy-targeted procedure among their non-Medicare patients. These novel findings demonstrate that Medicare rulemaking affects physician behavior beyond the program's statutory scope.
Keywords: Ambulatory surgery center; Healthcare regulation; Medicare; Physician.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Conflict of interest: We have not conflicts.
Figures
Similar articles
-
Ambulatory surgery centers--current legal issues 2004 (Part 2).Health Care Law Mon. 2004 May:3-10. Health Care Law Mon. 2004. PMID: 15188633
-
In the Shadow of a Giant: Medicare's Influence on Private Physician Payments.J Polit Econ. 2017 Feb;125(1):1-39. doi: 10.1086/689772. Epub 2016 Dec 16. J Polit Econ. 2017. PMID: 28713176 Free PMC article.
-
Treatment consolidation after vertical integration: Evidence from outpatient procedure markets.J Health Econ. 2022 Jan;81:102569. doi: 10.1016/j.jhealeco.2021.102569. Epub 2021 Nov 27. J Health Econ. 2022. PMID: 34911008 Free PMC article.
-
Interventional techniques in ambulatory surgical centers: a look at the new payment system.Pain Physician. 2007 Sep;10(5):627-50. Pain Physician. 2007. PMID: 17876360 Review.
-
Ambulatory surgery centers and interventional techniques: a look at long-term survival.Pain Physician. 2011 Mar-Apr;14(2):E177-215. Pain Physician. 2011. PMID: 21412380 Review.
Cited by
-
Physician responses to Medicare reimbursement rates.J Health Econ. 2023 Dec;92:102816. doi: 10.1016/j.jhealeco.2023.102816. Epub 2023 Oct 24. J Health Econ. 2023. PMID: 37883883 Free PMC article.
-
Private equity and healthcare firm behavior: Evidence from ambulatory surgery centers.J Health Econ. 2023 Sep;91:102801. doi: 10.1016/j.jhealeco.2023.102801. Epub 2023 Aug 6. J Health Econ. 2023. PMID: 37657144 Free PMC article.
-
Hospital behavior over the private equity life cycle.J Health Econ. 2024 Sep;97:102902. doi: 10.1016/j.jhealeco.2024.102902. Epub 2024 May 29. J Health Econ. 2024. PMID: 38861907
-
Lessons from health insurance responses in counteracting COVID-19: a qualitative comparative analysis of South Korea and three influential countries.Arch Public Health. 2023 Nov 21;81(1):205. doi: 10.1186/s13690-023-01209-w. Arch Public Health. 2023. PMID: 37990238 Free PMC article.
-
Fitting in? Physician practice style after forced relocation.Health Serv Res. 2024 Aug;59(4):e14340. doi: 10.1111/1475-6773.14340. Epub 2024 Jun 17. Health Serv Res. 2024. PMID: 38886564 Free PMC article.
References
-
- Baker LC, Bundorf MK, Kessler DP, 2019. Competition in outpatient procedure markets. Med. Care 57 (1), 36–41. - PubMed
-
- Barnett ML, Olenski A, and Sacarny A. 2020. “Common practice: spillovers from Medicare on private health care.” NBER Working Paper Series, w27270, http://www.nber.org/papers/w27270.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
