

Human liver single nucleus and single cell RNA sequencing identify a hepatocellular carcinoma-associated cell-type affecting survival
- PMID: 35581624
- PMCID: PMC9115949
- DOI: 10.1186/s13073-022-01055-5
Human liver single nucleus and single cell RNA sequencing identify a hepatocellular carcinoma-associated cell-type affecting survival
Abstract
Background: Hepatocellular carcinoma (HCC) is a common primary liver cancer with poor overall survival. We hypothesized that there are HCC-associated cell-types that impact patient survival.
Methods: We combined liver single nucleus (snRNA-seq), single cell (scRNA-seq), and bulk RNA-sequencing (RNA-seq) data to search for cell-type differences in HCC. To first identify cell-types in HCC, adjacent non-tumor tissue, and normal liver, we integrated single-cell level data from a healthy liver cohort (n = 9 non-HCC samples) collected in the Strasbourg University Hospital; an HCC cohort (n = 1 non-HCC, n = 14 HCC-tumor, and n = 14 adjacent non-tumor samples) collected in the Singapore General Hospital and National University; and another HCC cohort (n = 3 HCC-tumor and n = 3 adjacent non-tumor samples) collected in the Dumont-UCLA Liver Cancer Center. We then leveraged these single cell level data to decompose the cell-types in liver bulk RNA-seq data from HCC patients' tumor (n = 361) and adjacent non-tumor tissue (n = 49) from the Cancer Genome Atlas (TCGA) multi-center cohort. For replication, we decomposed 221 HCC and 209 adjacent non-tumor liver microarray samples from the Liver Cancer Institute (LCI) cohort collected by the Liver Cancer Institute and Zhongshan Hospital of Fudan University.
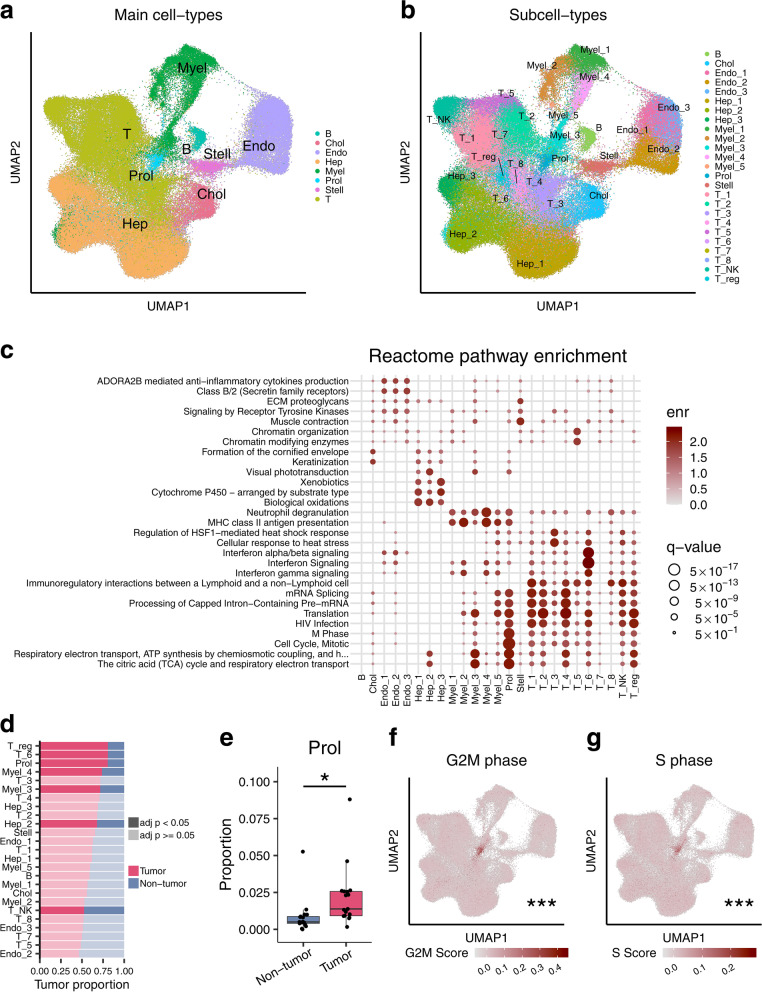
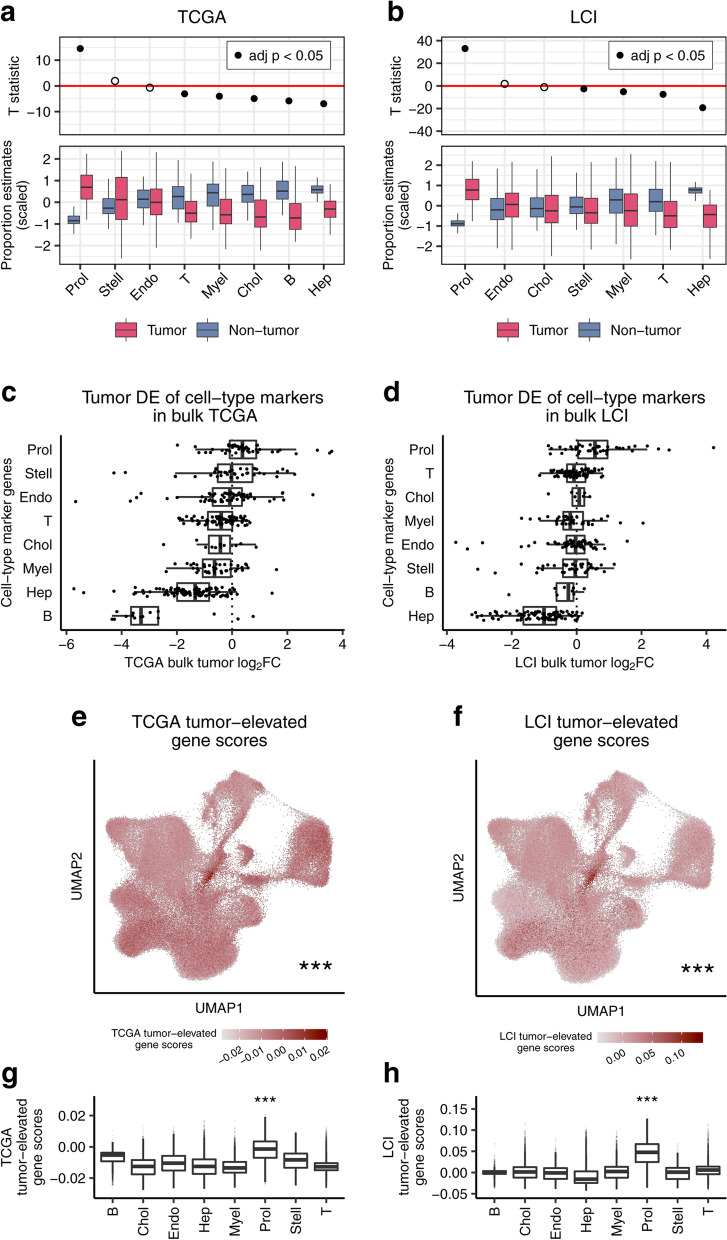
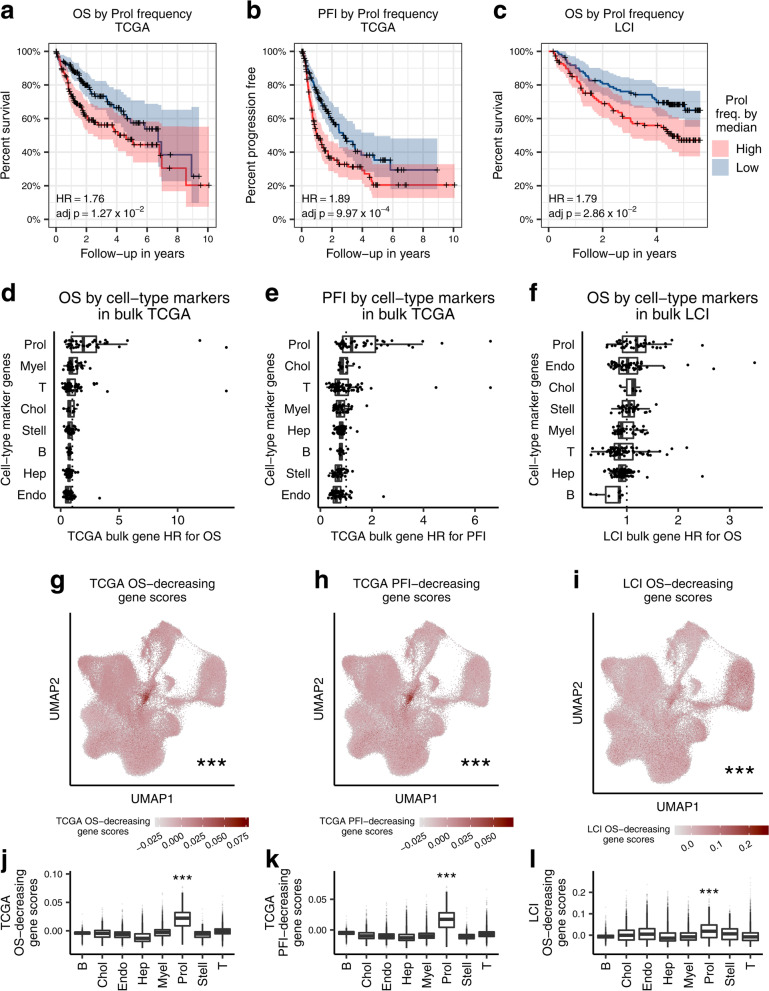
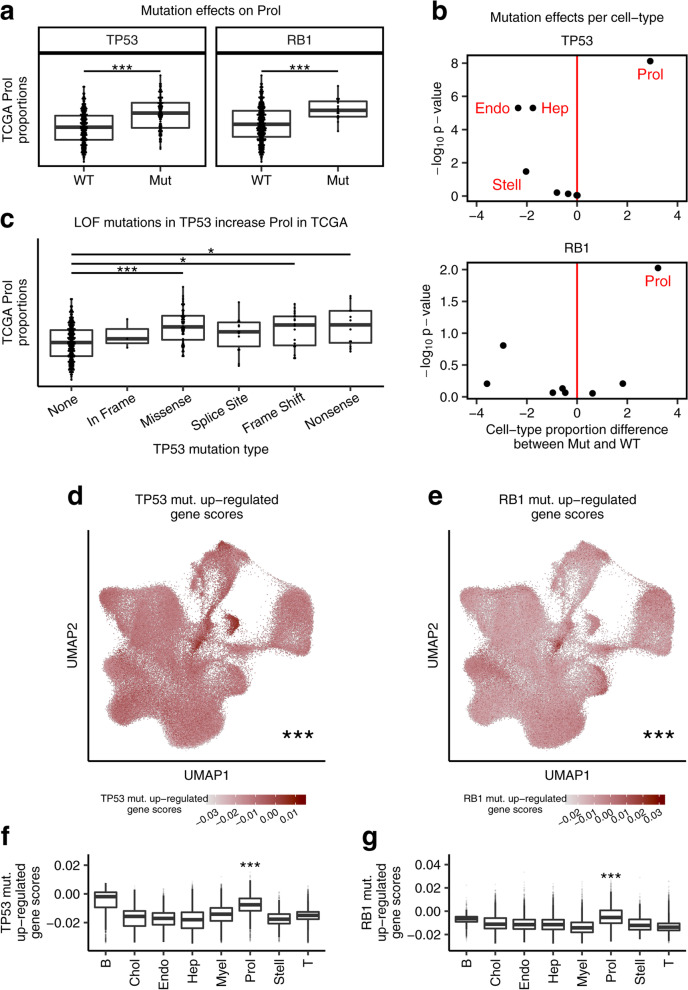
Results: We discovered a tumor-associated proliferative cell-type, Prol (80.4% tumor cells), enriched for cell cycle and mitosis genes. In the liver bulk tissue from the TCGA cohort, the proportion of the Prol cell-type is significantly increased in HCC and associates with a worse overall survival. Independently from our decomposition analysis, we reciprocally show that Prol nuclei/cells significantly over-express both tumor-elevated and survival-decreasing genes obtained from the bulk tissue. Our replication analysis in the LCI cohort confirmed that an increased estimated proportion of the Prol cell-type in HCC is a significant marker for a shorter overall survival. Finally, we show that somatic mutations in the tumor suppressor genes TP53 and RB1 are linked to an increase of the Prol cell-type in HCC.
Conclusions: By integrating liver single cell, single nucleus, and bulk expression data from multiple cohorts we identified a proliferating cell-type (Prol) enriched in HCC tumors, associated with a decreased overall survival, and linked to TP53 and RB1 somatic mutations.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
