

Prioritising attributes for tuberculosis preventive treatment regimens: a modelling analysis
- PMID: 35581650
- PMCID: PMC9115962
- DOI: 10.1186/s12916-022-02378-1
Prioritising attributes for tuberculosis preventive treatment regimens: a modelling analysis
Abstract
Background: Recent years have seen important improvements in available preventive treatment regimens for tuberculosis (TB), and research is ongoing to develop these further. To assist with the formulation of target product profiles for future regimens, we examined which regimen properties would be most influential in the epidemiological impact of preventive treatment.
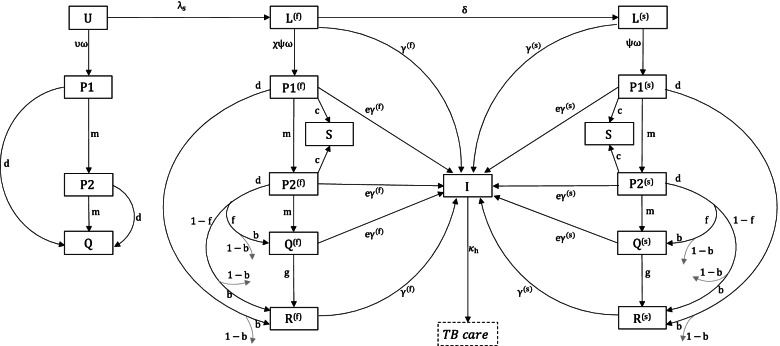
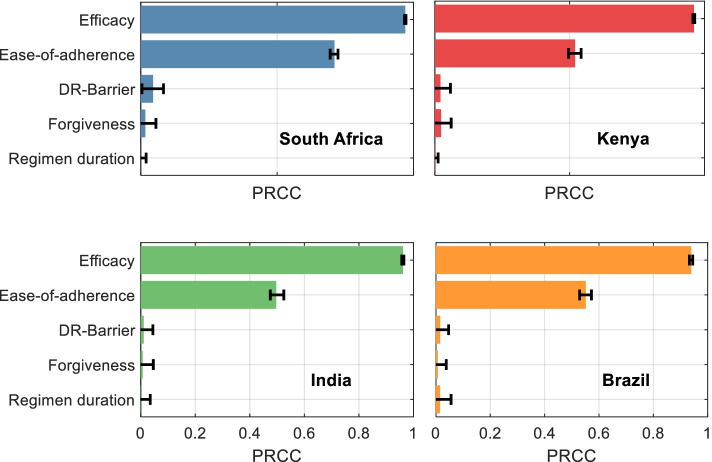
Methods: Following expert consultation, we identified 5 regimen properties relevant to the incidence-reducing impact of a future preventive treatment regimen: regimen duration, efficacy, ease-of-adherence (treatment completion rates in programmatic conditions), forgiveness to non-completion and the barrier to developing rifampicin resistance during treatment. For each regimen property, we elicited expert input for minimally acceptable and optimal (ideal-but-feasible) performance scenarios for future regimens. Using mathematical modelling, we then examined how each regimen property would influence the TB incidence reduction arising from full uptake of future regimens according to current WHO guidelines, in four countries: South Africa, Kenya, India and Brazil.
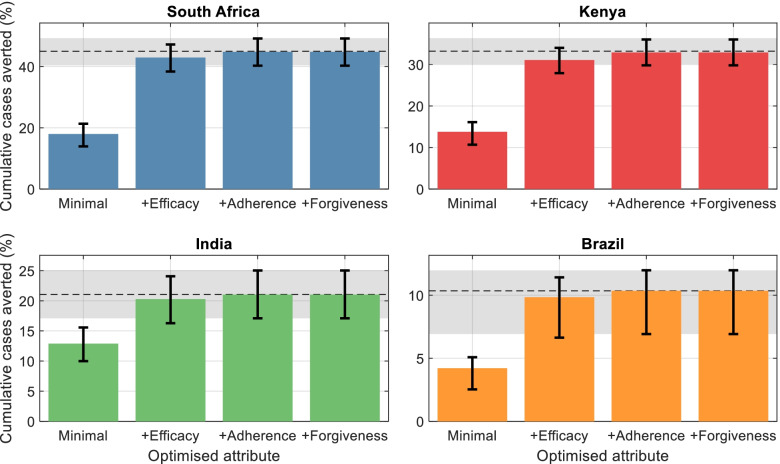
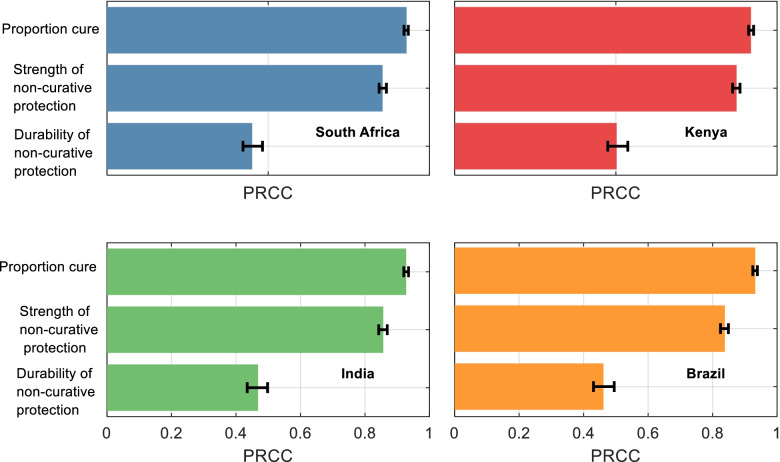
Results: Of all regimen properties, efficacy is the single most important predictor of epidemiological impact, while ease-of-adherence plays an important secondary role. These results are qualitatively consistent across country settings; sensitivity analyses show that these results are also qualitatively robust to a range of model assumptions, including the mechanism of action of future preventive regimens.
Conclusions: As preventive treatment regimens against TB continue to improve, understanding the key drivers of epidemiological impact can assist in guiding further development. By meeting these key targets, future preventive treatment regimens could play a critical role in global efforts to end TB.
Keywords: Mathematical modelling; Preventive therapy; Tuberculosis.
© 2022. The Author(s).
Conflict of interest statement
The authors have declared that they have no competing interests.
Figures
Similar articles
-
Scaling up target regimens for tuberculosis preventive treatment in Brazil and South Africa: An analysis of costs and cost-effectiveness.PLoS Med. 2022 Jun 13;19(6):e1004032. doi: 10.1371/journal.pmed.1004032. eCollection 2022 Jun. PLoS Med. 2022. PMID: 35696431 Free PMC article.
-
Priority-Setting for Novel Drug Regimens to Treat Tuberculosis: An Epidemiologic Model.PLoS Med. 2017 Jan 3;14(1):e1002202. doi: 10.1371/journal.pmed.1002202. eCollection 2017 Jan. PLoS Med. 2017. PMID: 28045934 Free PMC article.
-
Economic implications of novel regimens for tuberculosis treatment in three high-burden countries: a modelling analysis.Lancet Glob Health. 2024 Jun;12(6):e995-e1004. doi: 10.1016/S2214-109X(24)00088-3. Lancet Glob Health. 2024. PMID: 38762299 Free PMC article.
-
Shortened treatment regimens versus the standard regimen for drug-sensitive pulmonary tuberculosis.Cochrane Database Syst Rev. 2019 Dec 12;12(12):CD012918. doi: 10.1002/14651858.CD012918.pub2. Cochrane Database Syst Rev. 2019. PMID: 31828771 Free PMC article.
-
Tuberculosis.In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. 3rd edition. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2017 Nov 3. Chapter 11. PMID: 30212088 Free Books & Documents. Review.
Cited by
-
Scaling up target regimens for tuberculosis preventive treatment in Brazil and South Africa: An analysis of costs and cost-effectiveness.PLoS Med. 2022 Jun 13;19(6):e1004032. doi: 10.1371/journal.pmed.1004032. eCollection 2022 Jun. PLoS Med. 2022. PMID: 35696431 Free PMC article.
-
Tuberculosis Preventive Treatment in High TB-Burden Settings: A State-of-the-Art Review.Drugs. 2025 Feb;85(2):127-147. doi: 10.1007/s40265-024-02131-3. Epub 2024 Dec 28. Drugs. 2025. PMID: 39733063 Free PMC article. Review.
-
Factors Associated With Discontinuation of Tuberculosis Preventive Treatment: Post Hoc Analysis of 2 Randomized, Controlled Trials.Clin Infect Dis. 2023 Jul 5;77(1):84-93. doi: 10.1093/cid/ciad164. Clin Infect Dis. 2023. PMID: 36949623 Free PMC article. Clinical Trial.
References
-
- World Health Organization . Preventing TB. 2020.
-
- WHO. Latent TB infection: updated and consolidated guidelines for programmatic management. https://www.who.int/tb/publications/2018/latent-tuberculosis-infection/en/. Accessed 23 Apr 2020. - PubMed
-
- World Health Organization . Global tuberculosis report 2020. 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
