

Serum MOG-IgG in children meeting multiple sclerosis diagnostic criteria
- PMID: 35581944
- PMCID: PMC9442635
- DOI: 10.1177/13524585221093789
Serum MOG-IgG in children meeting multiple sclerosis diagnostic criteria
Abstract
Background: Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) is now recognized as distinct from multiple sclerosis (MS).
Objective: To evaluate the importance of considering myelin oligodendrocyte glycoprotein (MOG)-immunoglobulin-G (IgG) serology when applying MS diagnostic criteria in children.
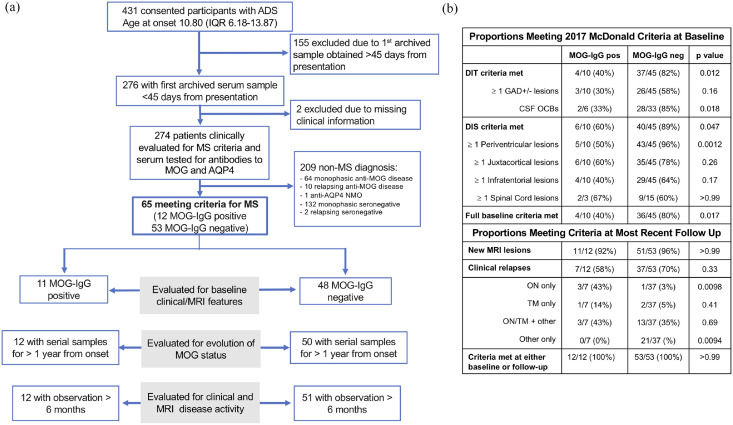
Methods: Within a prospective cohort of children meeting MS criteria (median follow-up = 6 years, interquartile range (IQR) = 4-9), we measured MOG-IgG in serial archived serum obtained from presentation, and compared imaging and clinical features between seropositive and seronegative participants.
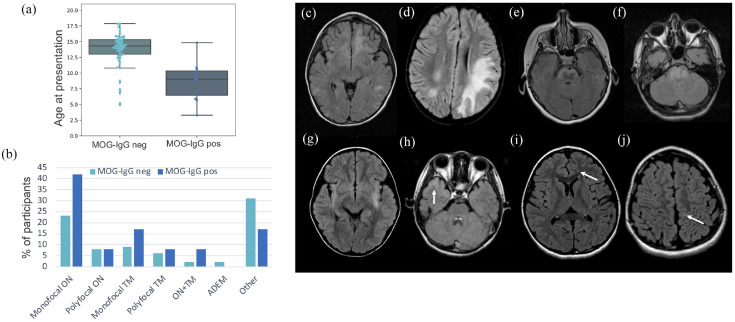
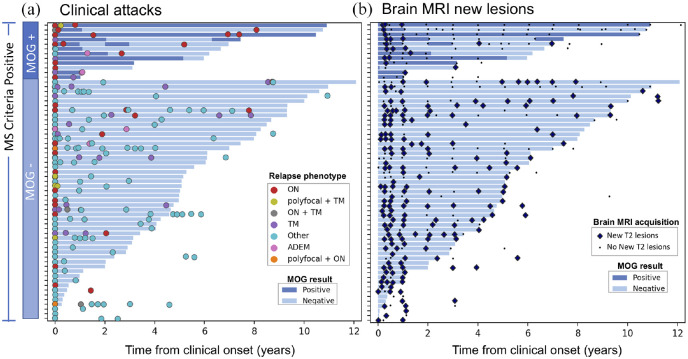
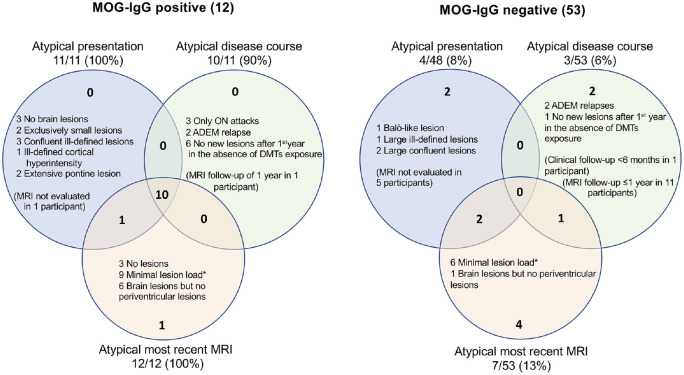
Results: Of 65 children meeting MS criteria (median age = 14.0 years, IQR = 10.9-15.1), 12 (18%) had MOG-IgG at disease onset. Seropositive participants were younger, had brain magnetic resonance imaging (MRI) features atypical for MS, rarely had cerebrospinal fluid (CSF) oligoclonal bands (2/8, 25%), and accumulated fewer T2 lesions over time. On serial samples, 5/12 (42%) were persistently seropositive, 5/12 (42%) became seronegative, and 2/12 (17%) had fluctuating results. All 12 children experienced a disease course different from typical MS.
Conclusion: While children with MOG-IgG can have clinical, CSF, and MRI features conforming to MS criteria, the presence of MOG-IgG is associated with atypical features and predicts a non-MS disease course. Given MOG-IgG seropositivity can wane over time, testing at first attack is of considerable importance for the diagnosis of MOGAD.
Keywords: All demyelinating diseases (CNS); MRI; all pediatric; autoimmune diseases; multiple sclerosis.
Conflict of interest statement
Figures
Similar articles
-
Assessment of international MOGAD diagnostic criteria in patients with overlapping MOG-associated disease and multiple sclerosis phenotypes.J Neurol. 2024 Sep;271(9):6160-6171. doi: 10.1007/s00415-024-12585-w. Epub 2024 Jul 27. J Neurol. 2024. PMID: 39066792
-
Immunoglobulin A Antibodies Against Myelin Oligodendrocyte Glycoprotein in a Subgroup of Patients With Central Nervous System Demyelination.JAMA Neurol. 2023 Sep 1;80(9):989-995. doi: 10.1001/jamaneurol.2023.2523. JAMA Neurol. 2023. PMID: 37548987 Free PMC article.
-
Myelin Oligodendrocyte Glycoprotein-Immunoglobulin G in the CSF: Clinical Implication of Testing and Association With Disability.Neurol Neuroimmunol Neuroinflamm. 2021 Oct 28;9(1):e1095. doi: 10.1212/NXI.0000000000001095. Print 2022 Jan. Neurol Neuroimmunol Neuroinflamm. 2021. PMID: 34711644 Free PMC article.
-
Clinical phenotype, radiological features, and treatment of myelin oligodendrocyte glycoprotein-immunoglobulin G (MOG-IgG) optic neuritis.Curr Opin Neurol. 2020 Feb;33(1):47-54. doi: 10.1097/WCO.0000000000000766. Curr Opin Neurol. 2020. PMID: 31743235 Review.
-
Myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD): current understanding and challenges.J Neurol. 2023 Aug;270(8):4132-4150. doi: 10.1007/s00415-023-11737-8. Epub 2023 May 8. J Neurol. 2023. PMID: 37154894 Free PMC article. Review.
Cited by
-
Radiological Features for Outcomes of MOGAD in Children: A Cohort in Southwest China.Neuropsychiatr Dis Treat. 2022 Aug 26;18:1875-1884. doi: 10.2147/NDT.S372446. eCollection 2022. Neuropsychiatr Dis Treat. 2022. PMID: 36052272 Free PMC article.
-
Multiple sclerosis in a 4-year-old boy: a case report and literature review.Front Neurol. 2024 Mar 22;15:1359938. doi: 10.3389/fneur.2024.1359938. eCollection 2024. Front Neurol. 2024. PMID: 38585366 Free PMC article.
-
Myelitis features and outcomes in CNS demyelinating disorders: Comparison between multiple sclerosis, MOGAD, and AQP4-IgG-positive NMOSD.Front Neurol. 2022 Nov 7;13:1011579. doi: 10.3389/fneur.2022.1011579. eCollection 2022. Front Neurol. 2022. PMID: 36419536 Free PMC article. Review.
-
Positive Predictive Value of MOG-IgG for Clinically Defined MOG-AD Within a Real-World Cohort.Front Neurol. 2022 Jun 20;13:947630. doi: 10.3389/fneur.2022.947630. eCollection 2022. Front Neurol. 2022. PMID: 35795797 Free PMC article.
-
Clinical characteristics of myelin oligodendrocyte glycoprotein antibody-associated disease according to their epitopes.Front Neurol. 2023 Jun 26;14:1200961. doi: 10.3389/fneur.2023.1200961. eCollection 2023. Front Neurol. 2023. PMID: 37435160 Free PMC article.
References
-
- Ketelslegers IA, Van Pelt DE, Bryde S, et al.. Anti-MOG antibodies plead against MS diagnosis in an acquired demyelinating syndromes cohort. Mult Scler 2015; 21(12): 1513–1520. - PubMed
-
- Hennes EM, Baumann M, Schanda K, et al.. Prognostic relevance of MOG antibodies in children with an acquired demyelinating syndrome. Neurology 2017; 89: 900–908. - PubMed
-
- Jurynczyk M, Geraldes R, Probert F, et al.. Distinct brain imaging characteristics of autoantibody-mediated CNS conditions and multiple sclerosis. Brain 2017; 140: 617–627. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
