

Evaluating the accuracy of American Society for Gastrointestinal Endoscopy guidelines in patients with acute gallstone pancreatitis with choledocholithiasis
- PMID: 35581962
- PMCID: PMC9048789
- DOI: 10.3748/wjg.v28.i16.1692
Evaluating the accuracy of American Society for Gastrointestinal Endoscopy guidelines in patients with acute gallstone pancreatitis with choledocholithiasis
Abstract
Background: Acute gallstone pancreatitis (AGP) is the most common cause of acute pancreatitis (AP) in the United States. Patients with AGP may also present with choledocholithiasis. In 2010, the American Society for Gastrointestinal Endoscopy (ASGE) suggested a management algorithm based on probability for choledocholithiasis, recommending additional imaging for patients at intermediate risk and endoscopic retrograde cholangiopancreatography (ERCP) for patients at high risk of choledocholithiasis. In 2019, the ASGE guidelines were updated using more specific criteria to categorize individuals at high risk for choledocholithiasis. Neither ASGE guideline has been studied in AGP to determine the probability of having choledocholithiasis.
Aim: To determine compliance with ASGE guidelines, assess outcomes, and compare 2019 vs 2010 ASGE criteria for suspected choledocholithiasis in AGP.
Methods: We conducted a retrospective cohort study of 882 patients admitted with AP to a single tertiary care center from 2008-2018. AP was diagnosed using revised Atlanta criteria and AGP was defined as the presence of gallstones on imaging or with cholestatic pattern of liver injury in the absence of another cause. Patients with chronic pancreatitis and pancreatic malignancy were excluded as were those who went directly to cholecystectomy prior to assessment for choledocholithiasis. Patients were assigned low, intermediate or high risk based on ASGE guidelines. Our primary outcomes of interest were the proportion of patients in the intermediate risk group undergoing magnetic resonance cholangiopancreatography (MRCP) first and the proportion of patients in the high risk group undergoing ERCP directly without preceding imaging. Secondary outcomes of interest included outcome differences based on if guidelines were not adhered to. We then evaluated the diagnostic accuracy of 2019 in comparison to the 2010 ASGE criteria for patients with suspected choledocholithiasis. We performed the t test or Wilcoxon rank sum test, as appropriate, to analyze if there were outcome differences based on if guidelines were not adhered to. Kappa coefficients were calculated to measure the degree of agreement between pairs of variables.
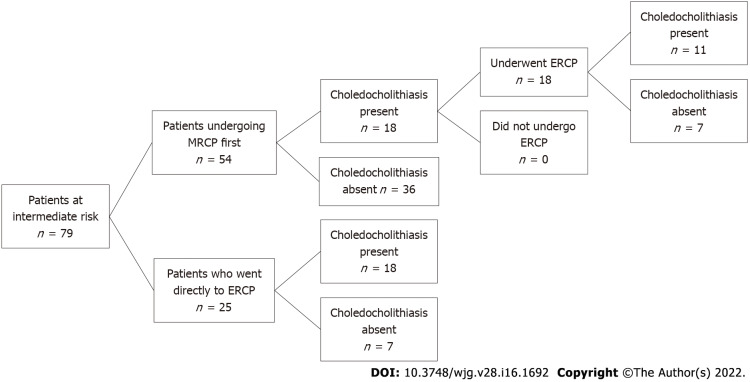
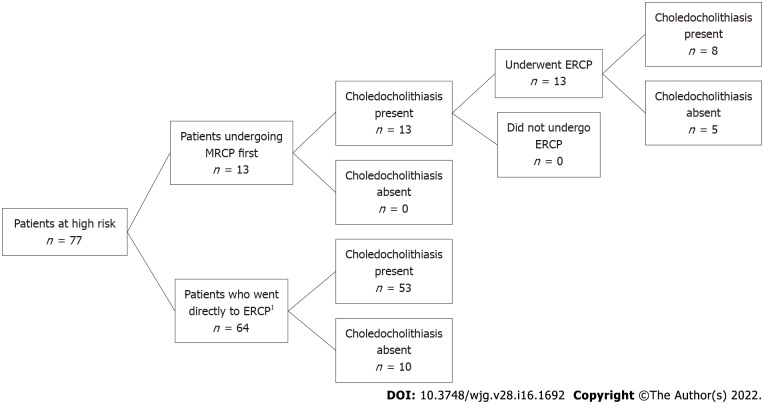
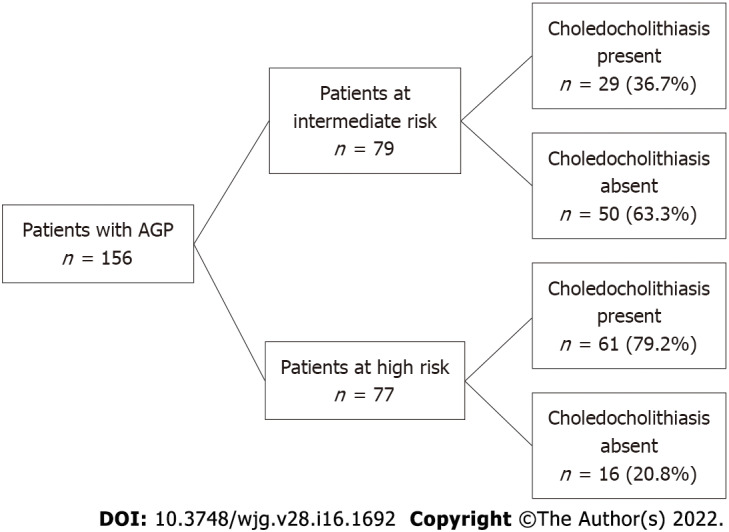
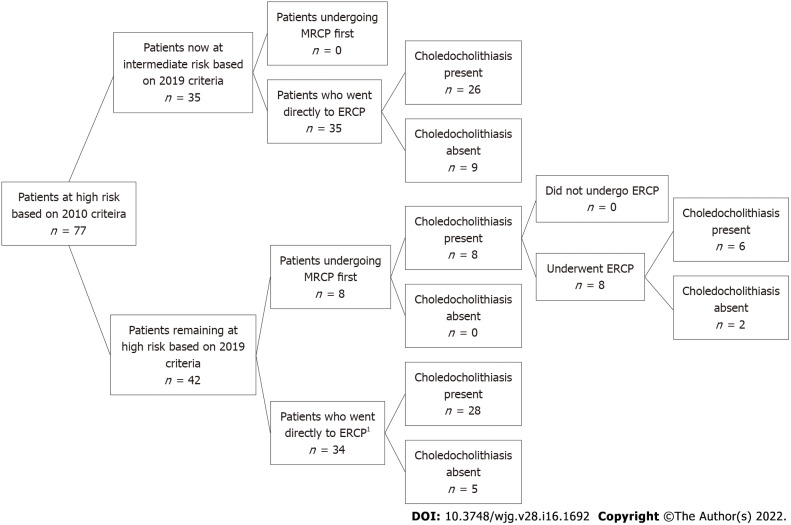
Results: In this cohort, we identified 235 patients with AGP of which 79 patients were excluded as they went directly to surgery for cholecystectomy without prior MRCP or ERCP. Of the remaining 156 patients, 79 patients were categorized as intermediate risk and 77 patients were high risk for choledocholithiasis according to the 2010 ASGE guidelines. Among 79 intermediate risk patients, 54 (68%) underwent MRCP first whereas 25 patients (32%) went directly to ERCP. For the 54 patients with intermediate risk who had MRCP first, 36 patients had no choledocholithiasis while 18 patients had evidence of choledocholithiasis prompting ERCP. Of these patients, ERCP confirmed stone disease in 11 patients. Of the 25 intermediate risk patients who directly underwent ERCP, 18 patients had stone disease. One patient with a normal ERCP developed post ERCP pancreatitis. Patients undergoing MRCP in this group had a significantly longer length of stay (5.0 vs 4.0 d, P = 0.02). In the high risk group, 64 patients (83%) had ERCP without preceding imaging, of which, 53 patients had findings consistent with choledocholithiasis, of which 13 patients (17%) underwent MRCP before ERCP, all of which showed evidence of stone disease. Furthermore, all of these patients ultimately had an ERCP, of which 8 patients had evidence of stones and 5 had normal examination.Our cohort also demonstrated that 58% of all 156 patients with AGP had confirmed choledocholithiasis (79% of the high risk group and 37% of the intermediate group when risk was assigned based on the 2010 ASGE guidelines). When the updated 2019 ASGE guidelines were applied instead of the original 2010 guidelines, there was moderate agreement between the 2010 and 2019 guidelines (kappa = 0.46, 95%CI: 0.34-0.58). Forty-two of 77 patients were still deemed to be high risk and 35 patients were downgraded to intermediate risk. Thirty-five patients who were originally assigned high risk were reclassified as intermediate risk. For these 35 patients, 26 patients had ERCP findings consistent with choledocholithiasis and 9 patients had a normal examination. Based on the 2019 criteria, 9/35 patients who were downgraded to intermediate risk had an unnecessary ERCP with normal findings (without a preceding MRCP).
Conclusion: Two-thirds in intermediate risk and 83% in high risk group followed ASGE guidelines for choledocholithiasis. One intermediate-group patient with normal ERCP had post-ERCP AP, highlighting the risk of unnecessary procedures.
Keywords: Acute gallstone pancreatitis; American Society for Gastrointestinal Endoscopy guidelines; Choledocholithiasis; Endoscopic retrograde cholangiopancreatography; Magnetic resonance cholangiopancreatography.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors of this study have no relevant conflict of interests to declare.
Figures
Similar articles
-
Performance of European and American Societies of Gastrointestinal Endoscopy Guidelines for Prediction of Choledocholithiasis in Patients with Acute Biliary Pancreatitis.Medicina (Kaunas). 2023 Dec 15;59(12):2176. doi: 10.3390/medicina59122176. Medicina (Kaunas). 2023. PMID: 38138279 Free PMC article.
-
Compliance to endoscopic retrograde cholangiopancreatography according to current guidelines and adverse outcomes of suspected choledocholithiasis in an acute care setting.Surg Endosc. 2022 Aug;36(8):5602-5609. doi: 10.1007/s00464-022-09113-0. Epub 2022 Mar 11. Surg Endosc. 2022. PMID: 35277770
-
The selective use of magnetic resonance cholangiopancreatography in the imaging of the axial biliary tree in patients with acute gallstone pancreatitis.Pancreatology. 2008;8(1):55-60. doi: 10.1159/000115667. Epub 2008 Feb 4. Pancreatology. 2008. PMID: 18253063
-
Utility of MRCP in clinical decision making of suspected choledocholithiasis: An institutional analysis and literature review.Am J Surg. 2017 Aug;214(2):251-255. doi: 10.1016/j.amjsurg.2016.10.025. Epub 2016 Dec 1. Am J Surg. 2017. PMID: 27986260 Review.
-
Systematic review and meta-analysis of the 2010 ASGE non-invasive predictors of choledocholithiasis and comparison to the 2019 ASGE predictors.Clin J Gastroenterol. 2022 Apr;15(2):286-300. doi: 10.1007/s12328-021-01575-4. Epub 2022 Jan 24. Clin J Gastroenterol. 2022. PMID: 35072902 Free PMC article.
Cited by
-
Performance of Diagnostic Guidelines in the Evaluation of Choledocholithiasis in Patients With Acute Biliary Presentation: A Systematic Review and Meta-Analysis.World J Surg. 2025 Aug;49(8):2153-2165. doi: 10.1002/wjs.12684. Epub 2025 Jun 26. World J Surg. 2025. PMID: 40569779 Free PMC article.
-
Performance of European and American Societies of Gastrointestinal Endoscopy Guidelines for Prediction of Choledocholithiasis in Patients with Acute Biliary Pancreatitis.Medicina (Kaunas). 2023 Dec 15;59(12):2176. doi: 10.3390/medicina59122176. Medicina (Kaunas). 2023. PMID: 38138279 Free PMC article.
References
-
- Forsmark CE, Baillie J AGA Institute Clinical Practice and Economics Committee; AGA Institute Governing Board. AGA Institute technical review on acute pancreatitis. Gastroenterology. 2007;132:2022–2044. - PubMed
-
- Rosseland AR, Glomsaker TB. Asymptomatic common bile duct stones. Eur J Gastroenterol Hepatol. 2000;12:1171–1173. - PubMed
-
- ASGE Standards of Practice Committee, Maple JT, Ben-Menachem T, Anderson MA, Appalaneni V, Banerjee S, Cash BD, Fisher L, Harrison ME, Fanelli RD, Fukami N, Ikenberry SO, Jain R, Khan K, Krinsky ML, Strohmeyer L, Dominitz JA. The role of endoscopy in the evaluation of suspected choledocholithiasis. Gastrointest Endosc. 2010;71:1–9. - PubMed
-
- Chandran A, Rashtak S, Patil P, Gottlieb A, Bernstam E, Guha S, Ramireddy S, Badillo R, DaVee RT, Kao LS, Thosani N. Comparing diagnostic accuracy of current practice guidelines in predicting choledocholithiasis: outcomes from a large healthcare system comprising both academic and community settings. Gastrointest Endosc. 2021;93:1351–1359. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
