

Comparative Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Serum Electrolyte Levels in Patients with Type 2 Diabetes: A Pairwise and Network Meta-Analysis of Randomized Controlled Trials
- PMID: 35582188
- PMCID: PMC9034808
- DOI: 10.34067/KID.0006672021
Comparative Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Serum Electrolyte Levels in Patients with Type 2 Diabetes: A Pairwise and Network Meta-Analysis of Randomized Controlled Trials
Abstract
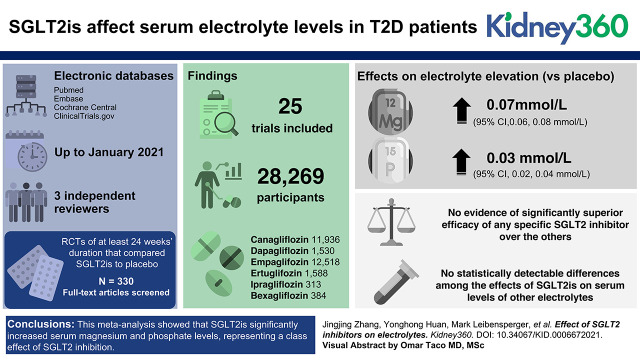
Background: Previous studies have reported that sodium-glucose co-transporter 2 (SGLT2) inhibitors (SGLT2is) affect levels of serum electrolytes, especially magnesium. This study aimed to integrate direct and indirect trial evidence to maximize statistical power to clarify their overall and comparative effects in patients with type 2 diabetes (T2D).
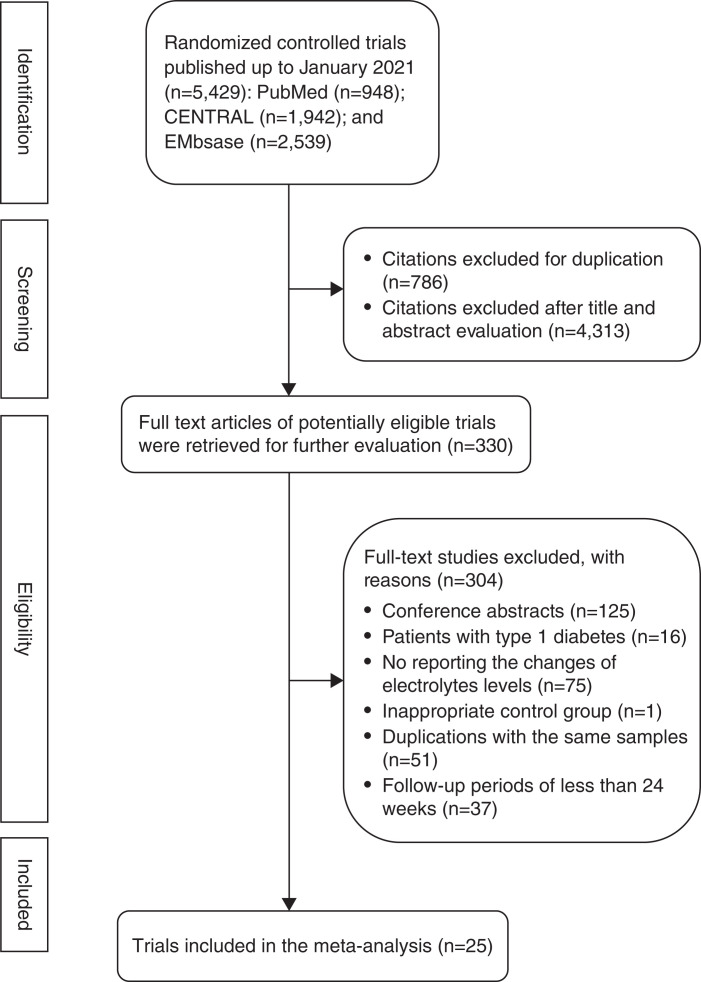
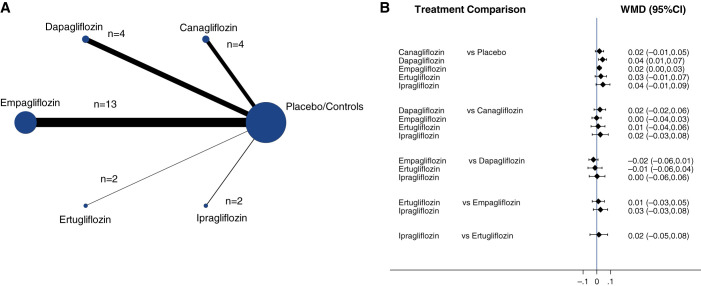
Methods: We systematically searched PubMed, EMBASE, CENTRAL, and ClinicalTrials.gov up to January 2021 to identify eligible randomized controlled trials (RCTs) of SGLT2is that reported mean changes in serum electrolytes, including magnesium, sodium, potassium, phosphate, and calcium. We performed both random-effects pairwise and network meta-analyses to calculate the weighted mean difference (WMD) and 95% confidence intervals (CI).
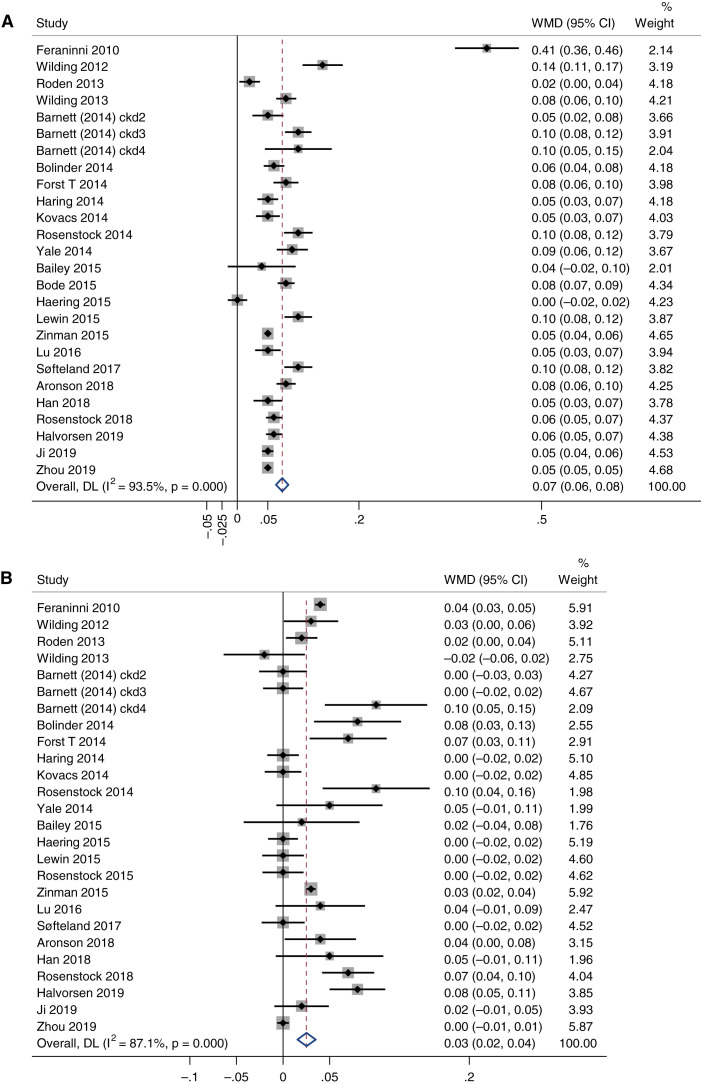
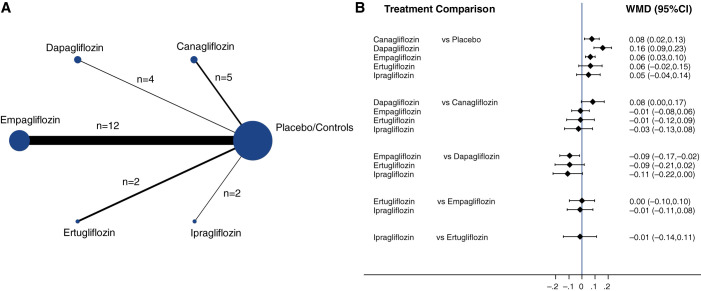
Results: In total, we included 25 RCTs involving 28,269 patients with T2D and 6 SGLT2is. Compared with placebo, SGLT2is were significantly associated with elevations in serum magnesium by 0.07 mmol/L (95% CI, 0.06 to 0.08 mmol/L) and serum phosphate by 0.03 mmol/L (95% CI, 0.02 to 0.04 mmol/L). Our network meta-analysis showed no evidence of significantly superior efficacy of any specific SGLT2 inhibitor over the others, although dapagliflozin was associated with a larger increment in serum magnesium (WMD=0.16 mmol/L) compared with other SGLT2is. Similarly, no statistically detectable differences among the effects of SGLT2is on serum levels of other electrolytes were detected.
Conclusions: SGLT2is significantly increased serum magnesium and phosphate levels, consistent with a class effect of SGLT2 inhibition. However, further investigations of long-term efficacy and safety in patients with T2D with different clinical phenotypes are needed.
Keywords: SGLT2 inhibitor; calcium; diabetes and the kidney; diabetes mellitus; electrolytes; magnesium; meta-analysis; phosphate; potassium; sodium; type 2 diabetes.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
All authors have nothing to disclose.
Figures
References
-
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS; DECLARE–TIMI 58 Investigators : Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 380: 347–357, 2019. 10.1056/NEJMoa1812389 - DOI - PubMed
-
- Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, Edwards R, Agarwal R, Bakris G, Bull S, Cannon CP, Capuano G, Chu PL, de Zeeuw D, Greene T, Levin A, Pollock C, Wheeler DC, Yavin Y, Zhang H, Zinman B, Meininger G, Brenner BM, Mahaffey KW; CREDENCE Trial Investigators : Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 380: 2295–2306, 2019. 10.1056/NEJMoa1811744 - DOI - PubMed
-
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, Mann JFE, McMurray JJV, Lindberg M, Rossing P, Sjöström CD, Toto RD, Langkilde AM, Wheeler DC; DAPA-CKD Trial Committees and Investigators : Dapagliflozin in patients with chronic kidney disease. N Engl J Med 383: 1436–1446, 2020. 10.1056/NEJMoa2024816 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
