

Pathologically Verified Corticobasal Degeneration Mimicking Richardson's Syndrome Coexisting with Clinically and Radiologically Shunt-Responsive Normal Pressure Hydrocephalus
- PMID: 35582317
- PMCID: PMC9092758
- DOI: 10.1002/mdc3.13442
Pathologically Verified Corticobasal Degeneration Mimicking Richardson's Syndrome Coexisting with Clinically and Radiologically Shunt-Responsive Normal Pressure Hydrocephalus
Abstract
Background: Normal pressure hydrocephalus (NPH) manifests as gait instability, cognitive impairment, and urinary incontinence. This clinical triad of NPH sometimes occurs with ventriculomegaly in patients with neurodegenerative disease. Patients with pathologically verified neurodegenerative diseases, such as progressive supranuclear palsy (PSP), have received antemortem diagnoses of NPH.
Objectives: This study presents clinical and pathological features of a patient with pathologically verified corticobasal degeneration (CBD) coexisting with clinically shunt-responsive NPH.
Methods: We performed clinical, radiological, and pathological evaluations in a patient with CBD whose antemortem diagnosis was PSP Richardson's syndrome (PSP-RS) coexisting with shunt-responsive NPH.
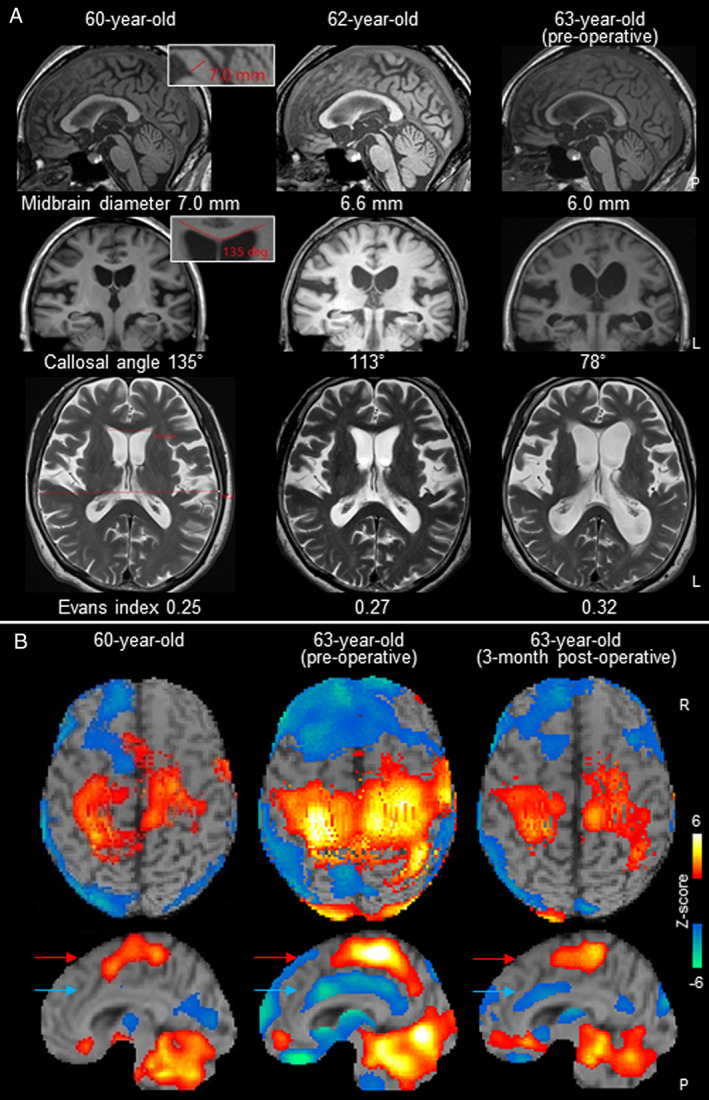
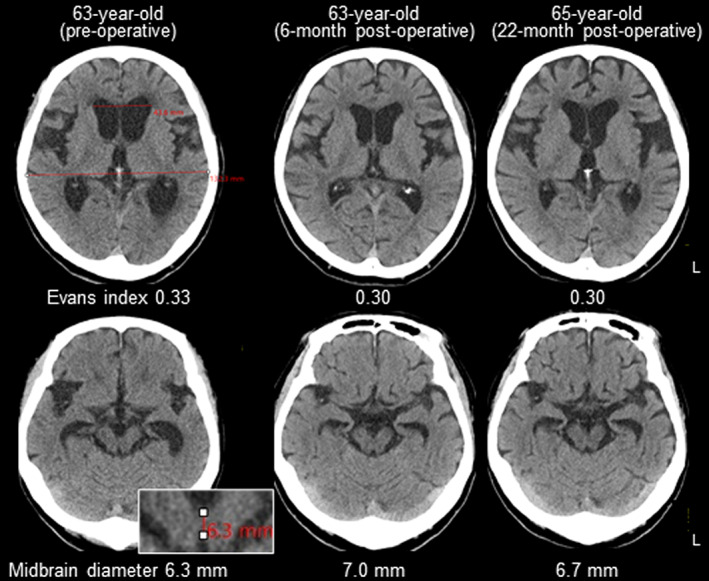
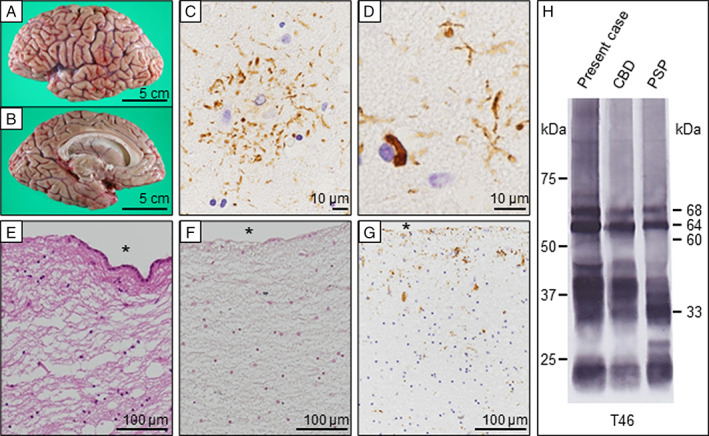
Results: A 59-year-old woman developed bradykinesia and gait instability and then frequent falls, urinary incontinence, and supranuclear vertical gaze palsy followed. At 63 years of age, her gait disturbance and urinary incontinence had deteriorated rapidly, and cognitive impairment was disclosed. There were typical findings of NPH with ventriculomegaly and disproportionately enlarged subarachnoid space hydrocephalus as well as a 2-layer appearance with decreased and increased cerebral blood perfusion. Shunt placement ameliorated gait instability for more than 1 year and improved radiological indicators of NPH. However, atrophy of the midbrain progressed with time after transient increases in size. Although the antemortem diagnosis was probable PSP-RS, pathological evaluation verified CBD. There were severe discontinuities of the ependymal lining of the lateral ventricles and subependymal rarefaction and gliosis with tau-positive deposition.
Conclusions: Shunt surgery could ameliorate NPH symptoms in patients with 4-repeat tauopathies. Careful assessments of clinical findings are necessary to predict the benefits of shunts as a therapeutic option for patients with neurodegenerative diseases coexisting with NPH.
Keywords: corticobasal degeneration; neurodegenerative NPH; normal pressure hydrocephalus; progressive supranuclear palsy; shunt surgery.
© 2022 The Authors. Movement Disorders Clinical Practice published by Wiley Periodicals LLC. on behalf of International Parkinson and Movement Disorder Society.
Figures
Similar articles
-
Progressive supranuclear palsy.Int Rev Neurobiol. 2019;149:49-86. doi: 10.1016/bs.irn.2019.10.013. Epub 2019 Nov 21. Int Rev Neurobiol. 2019. PMID: 31779824 Review.
-
Evaluation of disproportionately enlarged subarachnoid-space hydrocephalus in progressive supranuclear palsy.Brain Commun. 2025 Jun 3;7(3):fcaf206. doi: 10.1093/braincomms/fcaf206. eCollection 2025. Brain Commun. 2025. PMID: 40503329 Free PMC article.
-
Does corticobasal degeneration exist? A clinicopathological re-evaluation.Brain. 2010 Jul;133(Pt 7):2045-57. doi: 10.1093/brain/awq123. Brain. 2010. PMID: 20584946
-
Progressive supranuclear palsy with marked ventricular dilatation mimicking normal pressure hydrocephalus.Neurol Sci. 2022 Mar;43(3):1783-1790. doi: 10.1007/s10072-021-05594-4. Epub 2021 Sep 9. Neurol Sci. 2022. PMID: 34499242
-
Chameleons and mimics: Progressive supranuclear palsy and corticobasal degeneration.Neuropathology. 2020 Feb;40(1):57-67. doi: 10.1111/neup.12590. Epub 2019 Sep 12. Neuropathology. 2020. PMID: 31515852 Review.
Cited by
-
Disproportionately Enlarged Subarachnoid-Space Hydrocephalus on MRI in Pathologically Confirmed Progressive Supranuclear Palsy.Neurol Clin Pract. 2025 Apr;15(2):e200431. doi: 10.1212/CPJ.0000000000200431. Epub 2025 Feb 20. Neurol Clin Pract. 2025. PMID: 40007723
-
Progressive supranuclear palsy can mimic idiopathic normal pressure hydrocephalus: A case series.J Neuropathol Exp Neurol. 2023 Nov 20;82(12):1033-1036. doi: 10.1093/jnen/nlad090. J Neuropathol Exp Neurol. 2023. PMID: 37944016 Free PMC article. No abstract available.
References
-
- Espay AJ, Da Prat GA, Dwivedi AK, et al. Deconstructing normal pressure hydrocephalus: Ventriculomegaly as early sign of neurodegeneration. Ann Neurol 2017;82(4):503–513. - PubMed
-
- Leinonen V, Koivisto AM, Savolainen S, et al. Post‐mortem findings in 10 patients with presumed normal‐pressure hydrocephalus and review of the literature. Neuropathol Appl Neurobiol 2012;38(1):72–86. - PubMed
-
- Kobayashi S, Tateno M, Utsumi K, Takahashi A, Morii H, Saito T. Two‐layer appearance on brain perfusion SPECT in idiopathic normal pressure hydrocephalus: A qualitative analysis by using easy Z‐score imaging system, eZIS. Dement Geriatr Cogn Disord 2009;28(4):330–337. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
