

Cardiac myxomas: A narrative review
- PMID: 35582466
- PMCID: PMC9048271
- DOI: 10.4330/wjc.v14.i4.206
Cardiac myxomas: A narrative review
Abstract
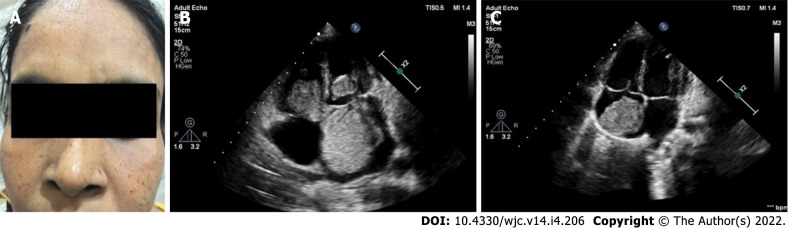
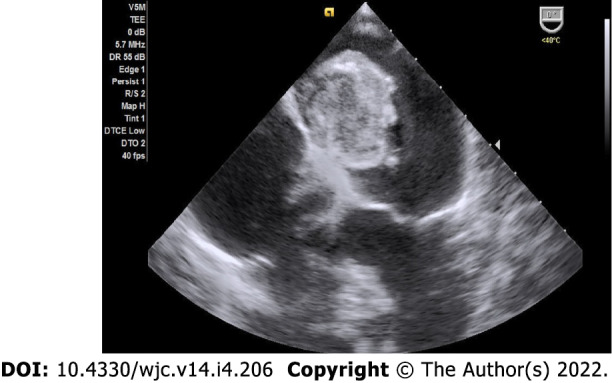
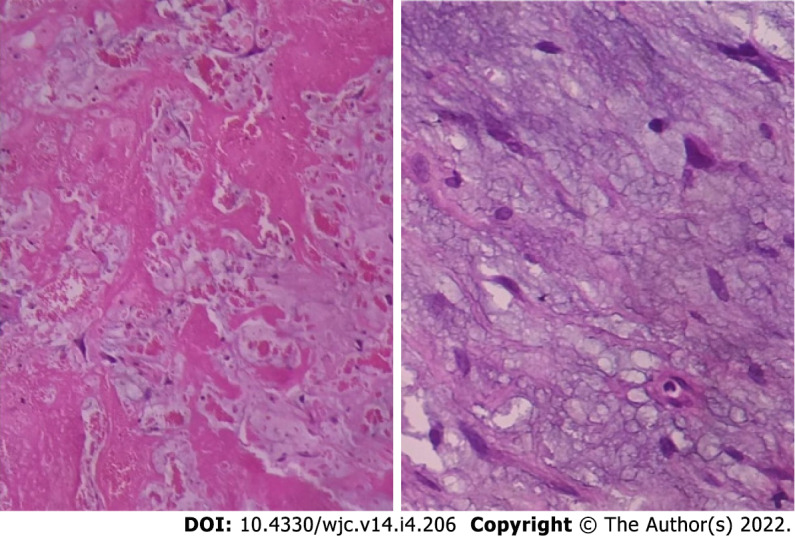
Cardiac myxomas are common primary neoplasms of the heart. They are biologically benign but "functionally malignant" because of the potential for embolization. They arise most commonly from the left atrium, but no chambers of the heart are immune. They may be sporadic in the majority but also familial as a part of the Carney complex. Two morphological forms exist: polypoid and papillary. Polypoid myxomas often present with obstructive features, while the papillary forms are more prone to embolization. Histogenesis is still controversial; the current view centres around origin from the primitive pluripotent mesenchymal cells. They may be of giant proportion, be calcified or get infected. Clinical presentation typically involves the triad of intracardiac obstruction, embolic events and constitutional symptoms. Precordial examination findings may simulate those of mitral or tricuspid stenosis. The presence of tumour plop and change of the physical findings with changing position may help differentiation between the two. Echocardiography is the investigation of choice. Echogenic polypoid or papillary mobile mass within the atrial cavity remaining attached to the interatrial septum through a stalk are the tell-tale echocardiographic features. Cardiac magnetic resonance and computed tomographic scanning may have incremental diagnostic value. Histopathological examination reveals abundant loose myxoid stroma with scattered round, polygonal or stellate cells with dense irregular nuclei. Genetic testing may detect mutations in the PRKAR1A gene in the familial form of cardiac myxoma, i.e. the Carney complex. Surgical excision is the mainstay of treatment with low operative mortality, excellent postoperative survival and low recurrence rate. The current trend favours minimal-access surgery with or without robotic assistance. Physicians should have appropriate preparedness to make a timely diagnosis and enthusiastic treatment to avoid potentially fatal complications.
Keywords: Cardiac; Carney Complex; Echocardiography; Embolism; Myxoma; Neoplasm.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare having no conflicts of interest.
Figures







References
-
- Velez Torres JM, Martinez Duarte E, Diaz-Perez JA, Rosenberg AE. Cardiac Myxoma: Review and Update of Contemporary Immunohistochemical Markers and Molecular Pathology. Adv Anat Pathol. 2020;27:380–384. - PubMed
-
- Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics. 2000;20:1073–103; quiz 1110. - PubMed
-
- Yoon DH, Roberts W. Sex distribution in cardiac myxomas. Am J Cardiol. 2002;90:563–565. - PubMed
-
- Keeling IM, Oberwalder P, Anelli-Monti M, Schuchlenz H, Demel U, Tilz GP, Rehak P, Rigler B. Cardiac myxomas: 24 years of experience in 49 patients. Eur J Cardiothorac Surg. 2002;22:971–977. - PubMed
-
- Pérez-Andreu J, Arribas Leal JM, Gervase G, Rivera-Caravaca JM, Cánovas López S, Marín F. Epidemiology of Cardiac Myxoma in a Spanish Population. A 30-year Surgical Series. Rev Esp Cardiol (Engl Ed) 2019;72:685–686. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
