

Mesentery solitary fibrous tumor with postoperative recurrence and sarcomatosis: A case report and review of literature
- PMID: 35582654
- PMCID: PMC9052071
- DOI: 10.5306/wjco.v13.i4.303
Mesentery solitary fibrous tumor with postoperative recurrence and sarcomatosis: A case report and review of literature
Abstract
Background: Solitary fibrous tumors are rare neoplasms of mesenchymal origin. They are often of low malignant potential and rarely metastasize. They frequently arise from the pleura and can occur at any soft tissue site in the body. However, these tumors rarely develop in the mesentery, peritoneal cavity or peritoneum.
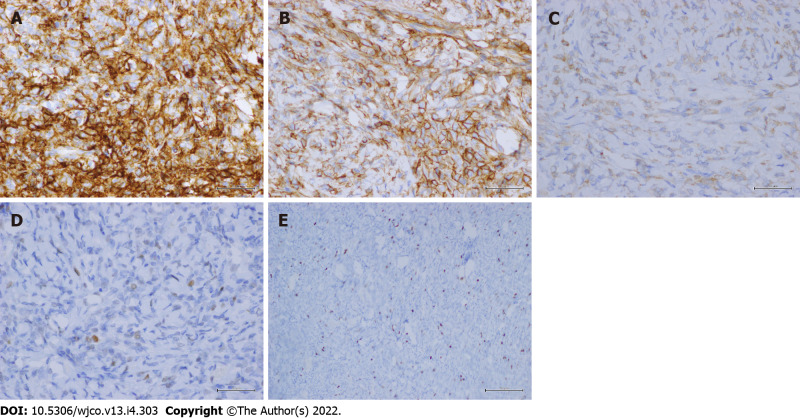
Case summary: We report on a scarce case of solitary fibrous tumor of the rectal mesentery showing sarcomatosis about 4 years after previous tumor resection. This 69-year-old male had no clinical symptoms but was transferred to our hospital because of a suspected tumor recurrence from follow-up abdominal computed tomography. Tumor markers (CEA, CA 19-9 and CA 125) were within the normal range. Open laparotomy showed sarcomatosis, and pathology confirmed its mesenchymal origin and diagnosis as the solitary fibrous tumor. Our case may be the second recurrent mesentery solitary fibrous tumor reported to date, and the only one with progression to sarcomatosis. There has been no evidence of recurrence in follow-up at the 28th mo after extensive intra-operative peritoneal lavage and cytoreductive surgery.
Conclusion: Although there are few risk factors of cancer recurrence in this patient, careful long-term follow-up after cytoreductive surgery is necessary.
Keywords: Case report; Cytoreductive surgery; Extensive intra-operative peritoneal lavage; Recurrence; Sarcomatosis; Solitary fibrous tumor of rectum mesentery.
©The Author(s) 2022. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures






Similar articles
-
Solitary fibrous tumor of the mesentery: a case report and review of the literature.J Int Med Res. 2020 Oct;48(10):300060520950111. doi: 10.1177/0300060520950111. J Int Med Res. 2020. PMID: 33050750 Free PMC article. Review.
-
Massive malignant solitary fibrous tumor arising from the bladder serosa: a case report.J Med Case Rep. 2015 Mar 1;9:46. doi: 10.1186/s13256-014-0505-4. J Med Case Rep. 2015. PMID: 25884588 Free PMC article. Review.
-
Solitary fibrous tumor arising in the mesentery: a case report.World J Surg Oncol. 2011 Oct 31;9:140. doi: 10.1186/1477-7819-9-140. World J Surg Oncol. 2011. PMID: 22035205 Free PMC article.
-
Solitary fibrous tumor of small bowel mesentery: a case report and review of the literature.Tumori. 2010 Nov-Dec;96(6):1035-9. Tumori. 2010. PMID: 21388072 Review.
-
A giant solitary fibrous tumor of the mesentery: a case report and literature review.World J Surg Oncol. 2015 Feb 4;13:17. doi: 10.1186/s12957-014-0422-4. World J Surg Oncol. 2015. PMID: 25649645 Free PMC article. Review.
Cited by
-
A giant solitary fibrous tumor of the abdominal pelvic cavity: A case report and literature review.Medicine (Baltimore). 2024 Aug 9;103(32):e39270. doi: 10.1097/MD.0000000000039270. Medicine (Baltimore). 2024. PMID: 39121255 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
