

Definitions and Standardized Endpoints for Treatment of Coronary Bifurcations
- PMID: 35583108
- PMCID: PMC10687650
- DOI: 10.4244/EIJ-E-22-00018
Definitions and Standardized Endpoints for Treatment of Coronary Bifurcations
Abstract
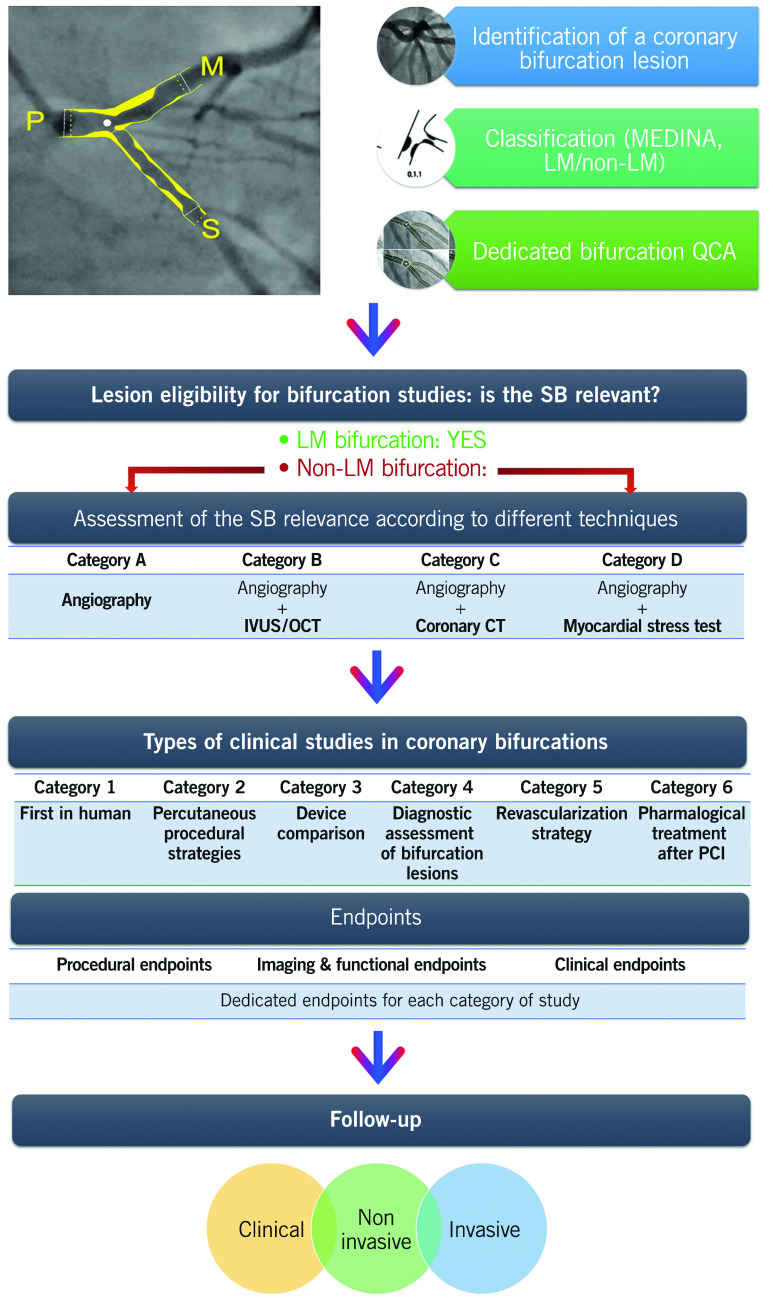
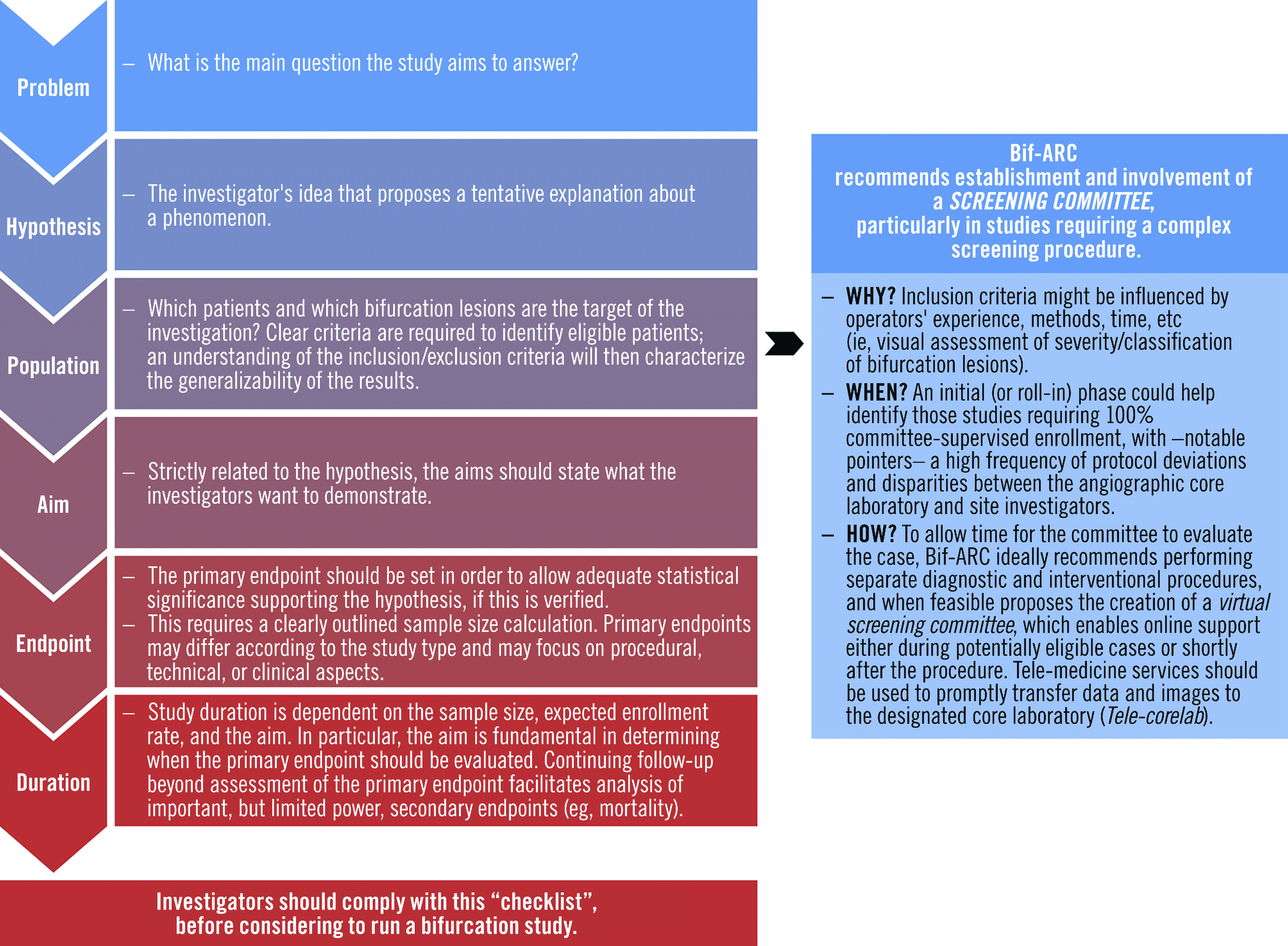
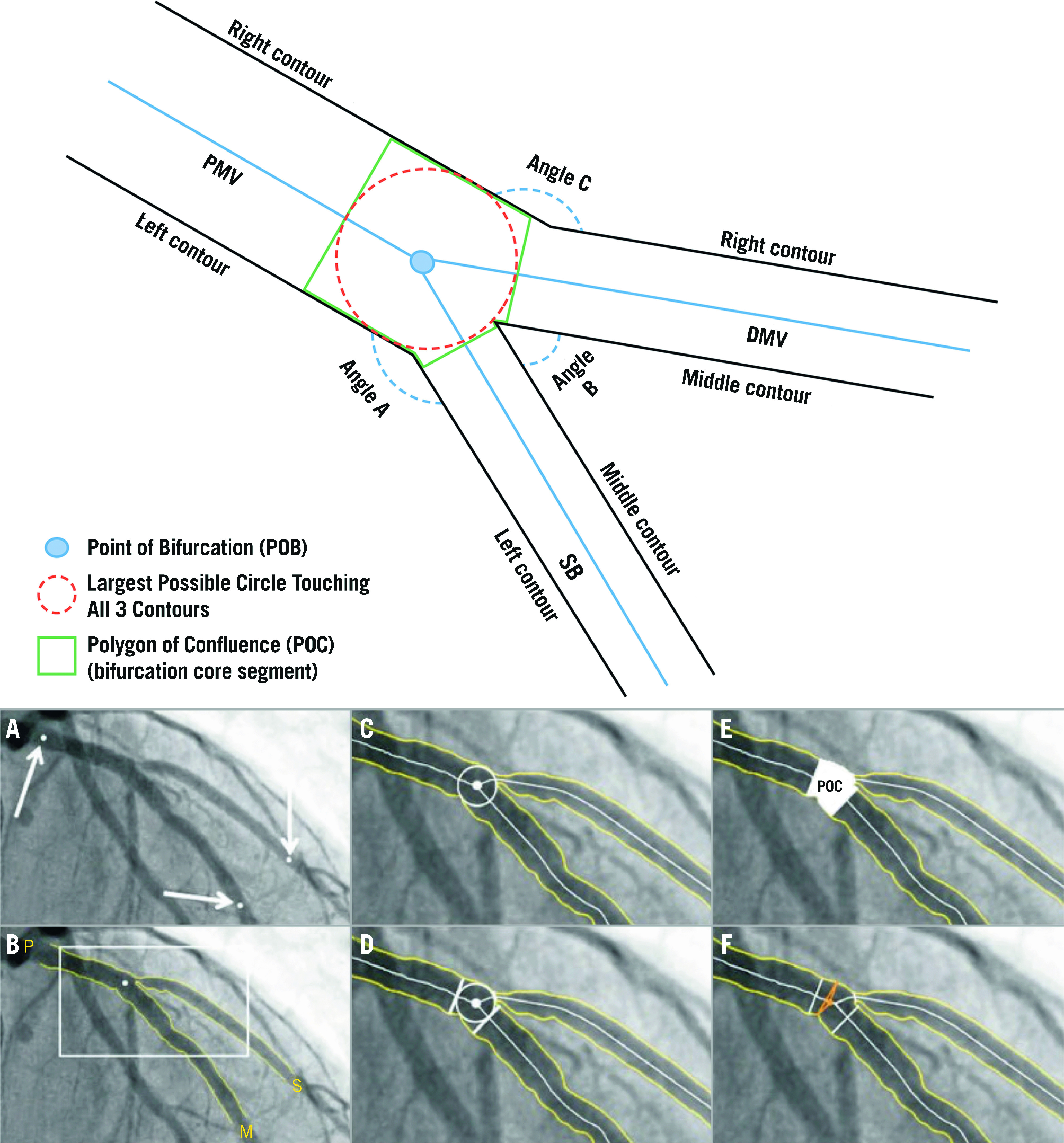
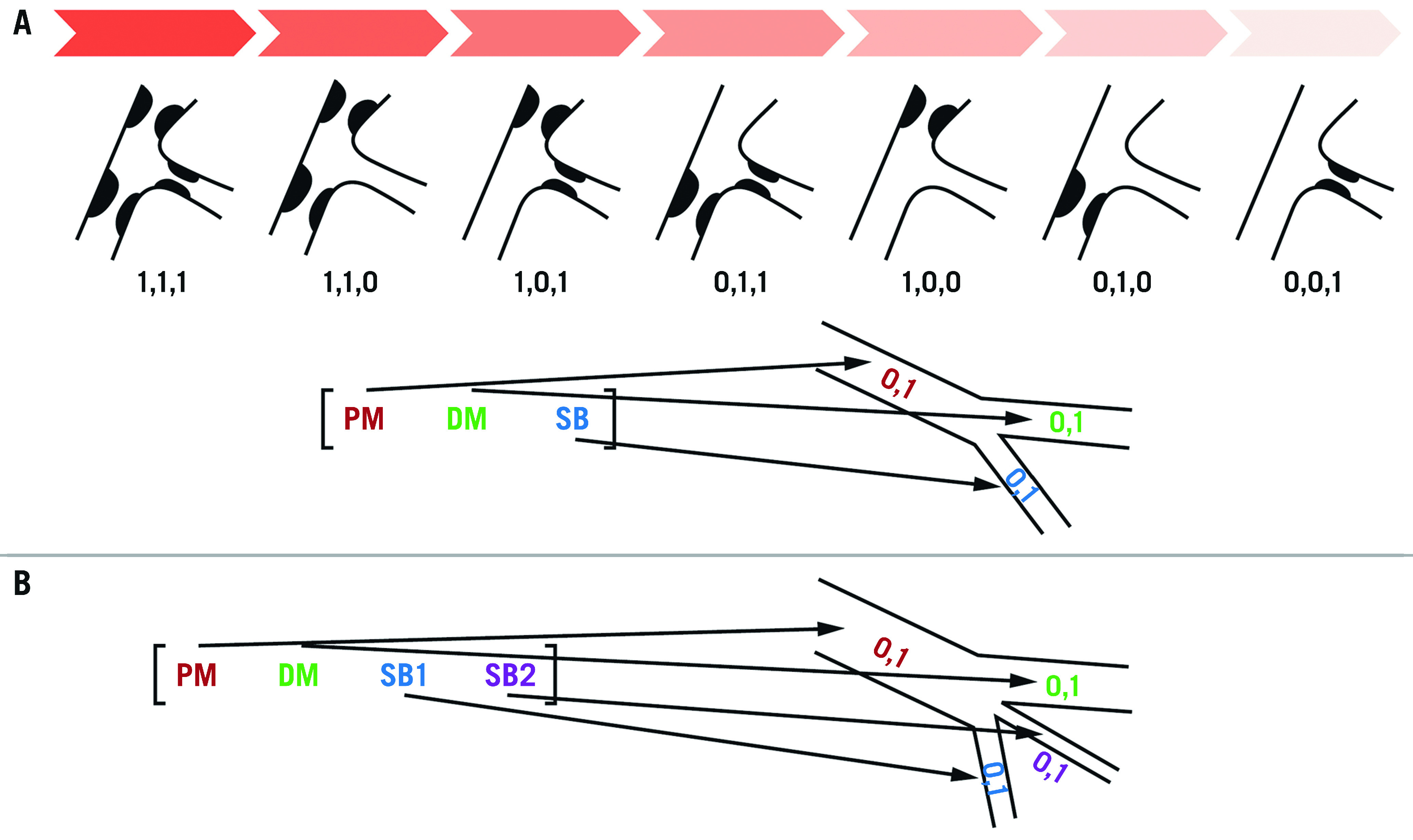
The Bifurcation Academic Research Consortium (Bif-ARC) project originated from the need to overcome the paucity of standardization and comparability between studies involving bifurcation coronary lesions. This document is the result of a collaborative effort between academic research organizations and the most renowned interventional cardiology societies focused on bifurcation lesions in Europe, the United States, and Asia. This consensus provides standardized definitions for bifurcation lesions; the criteria to judge the side branch relevance; the procedural, mechanistic, and clinical endpoints for every type of bifurcation study; and the follow-up methods. Considering the complexity of bifurcation lesions and their evaluation, detailed instructions and technical aspects for site and core laboratory analysis of bifurcation lesions are also reported. The recommendations included within this consensus will facilitate pooled analyses and the effective comparison of data in the future, improving the clinical relevance of trials in bifurcation lesions, and the quality of care in this subset of patients.
Conflict of interest statement
This work is supported by a Science Foundation Ireland Research Professorship Award (RSF 1413) including grants to Drs Lunardi and Wijns. Dr Lefèvre has received speaker fees from Abbott, Medtronic and Terumo. Dr Burzotta has received speaker fees from Medtronic, Abiomed, and Abbott. Dr Lassen has received speaker fees from Medtronic, Boston Scientific, Biotronik, Abbott and Biosensors. Dr Darremont has received speaker fees from Edwards. Dr Holm has received institutional research grants and speaker fees from St. Jude Medical and Terumo. -Dr -Johnson has received speaker fees from Abbott, Boston Scientific, Medtronic, and Terumo; and has received institutional funding for fellowships from Boston Scientific and Terumo. Dr Pan has received speaker fees from Abbott, Terumo, and Volcano. Dr -Chatzizisis has received speaker fees and consultation fees from Boston Scientific; and has received research support from Boston Scientific and Medtronic. Dr Banning has received institutional funding of a fellowship from Boston Scientific; and has received speaker fees from -Boston, Abbott, Medtronic, Philips/Volcano, and Miracor. Dr Chieffo has received speaker fees from Abiomed and GADA. Dr Dudek has received grants and personal fees from Boston Scientific, Philips, Abbott, Medtronic, and -Biotronik. Dr Hildick-Smith has received advisory board, consultancy, and research funding from Terumo, Medtronic, Abbott, and Boston Scientific. Dr Dangas has received lecture fees from Bayer and Daiichi--Sankyo; has received institutional and grant support from Daiichi-Sankyo; and has held equity in Medtronic. Dr Stone has received lecture fees from Terumo and Amaranth; has received consulting fees from Shockwave Medical, TherOx, Reva, Vascular Dynamics, Robocath, HeartFlow, Gore, Ablative Solutions, Matrizyme, Miracor Medical, Neovasc, V-Wave, Abiomed, Claret Medical, Sirtex Medical, MAIA Pharmaceuticals, VALFIX Medical, -SpectraWAVE, Ancora, and Vectorious Medical Technologies; holds equity in VALFIX Medical, Ancora, Qool Therapeutics, Orchestra BioMed, Cagent Vascular, Applied Therapeutics, -Biostar, MedFocus, Aria CV, Cardiac Success, and SpectraWAVE; holds stock options in Ancora, Qool Therapeutics, Orchestra BioMed, Cagent Vascular, Applied Therapeutics, Biostar, MedFocus, Aria CV, and Cardiac Success; and has received personal fees from Qool Therapeutics and Orchestra BioMed. Dr Cutlip has received grant support from Cordis; has received travel reimbursement from Abbott Vascular; and has received additional funding for the Clinical Events Committee from Boston Scientific. Dr Mehran has received institutional grant support from Abbott Laboratories, -AstraZeneca, Bayer, CSL Behring, Daiichi-Sankyo, Medtronic, Novartis, -Bristol Myers Squibb, and OrbusNeich; has received consulting fees from Abbott Laboratories (paid to her institution), -Spectranetics (Philips Volcano) (paid to her institution), Boston Scientific, -Medscape (WebMD), -Siemens Medical Solutions, -Roivant Services, Sanofi, Regeneron, and Janssen Scientific Affairs; has received lecture fees from Abbott Laboratories (paid to her institution), and Medtelligence (Janssen Scientific Affairs); has served on advisory boards for Bristol Myers Squibb (fees paid to her institution), PLx Opco, and Medtelligence (-Janssen Scientific Affairs); has served on a data and safety monitoring board (fees paid to her institution) for Watermark Research Partners; has received nonfinancial support from Regeneron; and holds equity in Claret Medical and Elixir Medical. Dr Wijns has received institutional research grants from Terumo, MiCell, and MicroPort; has received honoraria from MicroPort; has been a medical advisor of Rede Optimus Research; and is cofounder of Argonauts, an innovation accelerator. Dr Serruys has received personal fees from Philips/Volcano, SMT, Novartis, Xeltis, and Merillife. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Lassen JF, Burzotta F, Banning A, Lefèvre T, Darremont O, Hildick-Smith D, Chieffo A, Pan M, Holm NR, Louvard Y, Stankovic G. Percutaneous coronary intervention for the left main stem and other bifurcation lesions: 12th consensus document from the European Bifurcation Club. EuroIntervention. 2018;13:1540–53. - PubMed
-
- Burzotta F, Lassen JF, Lefèvre T, Banning AP, Chatzizisis YS, Johnson TW, Ferenc M, Rathore S, Albiero R, Pan M, Darremont O, Hildick-Smith D, Chieffo A, Zimarino M, Louvard Y, Stankovic G. Percutaneous coronary intervention for bifurcation coronary lesions: the 15th consensus document from the European Bifurcation Club. EuroIntervention. 2021;16:1307–17. - PMC - PubMed
-
- Medina A, Suárez de, Pan M. [A New Classification of Coronary Bifurcation Lesions]. Rev Esp Cardiol. 2006;59:183. [Article in Spanish]. - PubMed
-
- Perl L, Witberg G, Greenberg G, Vaknin-Assa H, Kornowski R, Assali A. Prognostic significance of the Medina classification in bifurcation lesion percutaneous coronary intervention with second-generation drug-eluting stents. Heart Vessels. 2020;35:331–9. - PubMed
-
- Legrand V, Thomas M, Zelízko M, De Bruyne B, Reifart N, Steigen T, Hildick-Smith D, Albiero R, Darremont O, Stankovic G, Pan M, Lassen JF, Louvard Y, Lefèvre T. Percutaneous coronary intervention of bifurcation lesions: state-of-the-art. Insights from the second meeting of the European Bifurcation Club. EuroIntervention. 2007;3:44–9. - PubMed