

Noninferiority Margin Size and Acceptance of Trial Results: Contingent Valuation Survey of Clinician Preferences for Noninferior Mortality
- PMID: 35583116
- PMCID: PMC9277322
- DOI: 10.1177/0272989X221099493
Noninferiority Margin Size and Acceptance of Trial Results: Contingent Valuation Survey of Clinician Preferences for Noninferior Mortality
Abstract
Objectives: We used modified contingent valuation methodology to determine how noninferiority margin sizes influence clinicians' willingness to accept clinical trial results that compare mortality in critically ill children.
Methods: We surveyed pediatric infectious diseases and critical care clinicians in Canada, Australia, and New Zealand and randomized respondents to review 1 of 9 mock abstracts describing a noninferiority trial of bacteremic critically ill children assigned to 7 or 14 d of antibiotics. Each scenario showed higher mortality in the 7-d group but met noninferiority criterion. We explored how noninferiority margins and baseline mortality rates influenced respondent acceptance of results.
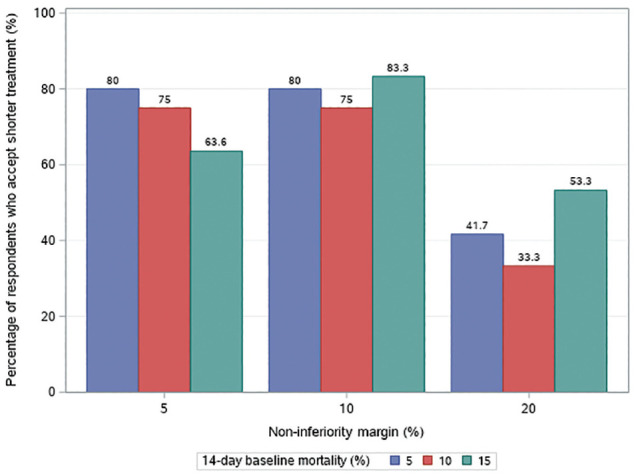
Results: There were 106 survey respondents: 65 (61%) critical care clinicians, 28 (26%) infectious diseases physicians, and 13 (12%) pharmacists. When noninferiority margins were 5% and 10%, 73% (24/33) and 79% (27/33) respondents would accept shorter treatment, compared with 44% (17/39) when the margin was 20% (P = 0.003). Logistic regression adjusted for baseline mortality showed 5% and 10% noninferiority margins were more likely to be associated with acceptance of shorter treatment compared with 20% margins (odds ratio [OR] 3.5, 95% confidence interval [CI]: 1.3-9.6, P = 0.013; OR 5.1, 95% CI: 1.8-14.6, P = 0.002). Baseline mortality was not a significant predictor of acceptance of shorter treatment.
Conclusions: Clinicians are more likely to accept shorter treatment when noninferiority margins are ≤10%. However, nearly half of respondents who reviewed abstracts with 20% margins were still willing to accept shorter treatment. This is a novel application of contingent valuation methodology to elicit acceptance of research results among end users of the medical literature.
Highlights: Clinicians are more likely to accept shorter treatment durations based on noninferior mortality results when the noninferiority margin is 5% or 10% than if the margin is 20%.However, nearly half of clinicians would still accept shorter-duration treatment as noninferior with margins of 20%.Baseline mortality does not independently predict acceptance of shorter-duration treatment.Contingent valuation is a novel approach to elicit the acceptance of research design parameters from the perspective of endusers of the medical literature.
Keywords: antimicrobials; contingent valuation; duration of therapy; evidence uptake; mortality; noninferiority margin.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was not funded. Sandra Pong is supported by a SickKids Clinician-Scientist Training Program Scholarship from The Hospital for Sick Children.
Figures
References
-
- Piaggio G, Elbourne DR, Altman DG, et al. Reporting of noninferiority and equivalence randomized trials: an extension of the CONSORT statement. JAMA. 2006;295:1152–60. - PubMed
-
- Mauri L, D’Agostino RB. Challenges in the design and interpretation of non-inferiority trials. N Engl J Med. 2017;377:1357–67. - PubMed
-
- Arrow K, Solow R, Portney P, et al. Report of the NOAA Panel on Contingent Valuation. Washington (DC): National Oceanic and Atmospheric Administration; 1993.
-
- O’Brien B, Gafni A. When do the “dollars” make sense? Towards a conceptual framework for contingent valuation studies in health care. Med Decis Making. 1996;16:288–99. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
